Download
1 / 70
710 likes | 1.11k Views
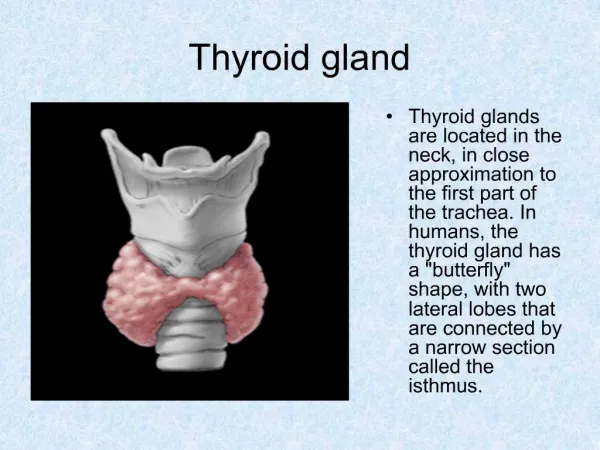
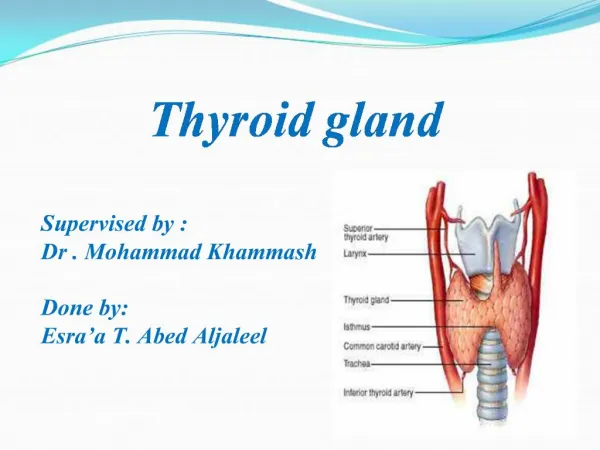
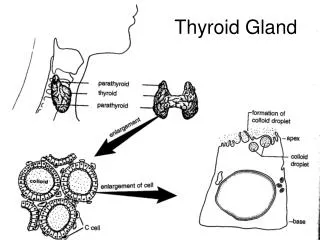
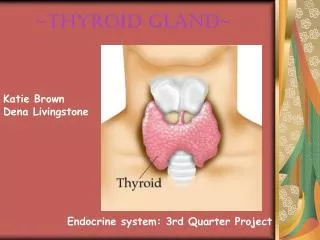
Thyroid gland diseases . Diffuse toxic goiter . hypothyreosis . Endemic goiter. Etiology . Clinical picture . Diagnostics . Complications . Principles of treatment . Thyrotoxic crisis . Hypothyreoid coma . Emergency care. Structure and location of thyroid gland.

E N D
Thyroid gland diseases. Diffuse toxic goiter. hypothyreosis. Endemic goiter. Etiology. Clinical picture. Diagnostics. Complications. Principles of treatment. Thyrotoxic crisis. Hypothyreoid coma. Emergency care
Physiological actions of thyroid hormones Protein metabolism– stimulation of protein synthesis;Carbohydratemetabolism – acceleration of their resorption from intestine and consumption by a liver;Fat metabolism - acceleration of lipolysis, cholsterol synthesis and metobolism;Liquid exchange - intensification of water evacuation by kidneysMineral homeostasis – regulation of Са, К, Р, Сl metabolism. Increased oxygen consumption with all tissues (except of brain tissue, spleen and testes); Increased heat production; Increased amount of catecholamine receptors in myocardium; Regulation of respiratory centre; Stimulation of erythropoiesis; Stimulation of bone tissue formation and resorption.
Influence of thyroid hormones on an organism: Nervous system and psychic Cardiovascular system Digestive system Reproductive system Skin and intertguments Musculosceletal apparatus
Endemic goitre This is a disease manifested with thyroid gland enlargement. It develops in certain biogeochemical regions characterized by iodine deficiency in the environment
Ethiology • Iodine deficiency is the main obvious factor • Additional factors: • deficiency of microelements cobalt, copper, fluorine, zinc, molybdenum (participate in iodine metabolism);Influence of strumogens – substances which decelerate biosynthesis of thyroid hormonesHypersecretionof thyrotrophic hormone (TTH) by hypophysis • Diseases of digestive tract, a liver with disordered iodine absorption.
Palpation of thyroid gland Position of patient is upright with relaxed neck muscles, the neck is slightly bended forward. Position of a doctor may be behind (I variant) or before the patient (II variant). A doctor performs palpation with tip of his fingers. In I variant of palpation examiner puts four fingers of both hands (except of thumbs) in projection of left and right parts of cricoid process. In II variant the examiner puts thumbs of his fingers in the same points (see next pictures). A patient is asked to swallow saliva (a gland goes up and becomes more accessible both a review and palpation). During swallowing doctor’s fingers slide across thyroid gland lobes and the isthmus. The following properties of the gland are to be assessed: location, pain, size, symmetry, consistency, structure (homogenous or with nodes).
Palpation may be performed, if a doctor stands behind or before the patient, his arms are put at the zone of projection of the gland
Diagnostics • 1. Anamnesis – residence in endemic region • 2. Palpation of thyroid gland – thyroid gland is enlarged, painless, homogenous, mild-elastic • 3. Level of thyroid hormones: Т4,Т3 - normal, ТТH normal or increased3. Ultrasound examination of thyroid gland
Treatment • 1. Thyroid hormones – L-thyroxin - 50-100 мcg/d;2. Iodinum preparations – 100-200 мcg/d • Prophylaxis of iodine defficiensy • Iodinum-containing products (salt, bred, milk); 2. Iodinum preparations:iodide potassium, lipiodol 100-200 мcg/d.
Epidemiology Spreadingof thyrotoxicosis is about 0,5 % DTG often develops in the age 20-50 years. Females develop this disease in 5-7 times more often than males Diffuse toxic goitre (DTG)
Ethiology and provoking factors • stress; • Infectious diseases; • insolation; • smocking; • Inflammatory processes in thyroid gland • Hormonal disbalance • heredity
Pathogenesis • Deficiency of T-supressors • CD4+, CD8+ • T- and B-lymphocytes recognizing thyroid gland antigens • antigenspecific stimulation of B-lymphocytes • Production of stimulating antibodies to TTH receptors
Clinical patternComplaints • Nervous system –tearfulness, depression, deranged sleep, irritability, oversweating Cardiovascular system – Permanent palpitation, periodical intermissions, dyspnea • Metabolism – poor tolerance to heat, low body weight while appetite is increased, muscular weakness Digestive tract - increasedappetite; abdominal pain; periodical diarrhoea Ophthalmopathy – feeling of protrusion of eyes, dacryagogue; photophobia Interguments – brittle hair, loosing hair.
Objective examination • Red dermographism. • Cardiovascular system – tachicardia, extrasystoly, atrial fibrillation; • Intensification of І heart sound, systolic murmur, • Heart failure; • Systolic arterial hypertension • Sex glands – Disorders of menstrual function and problems with pregnancy in females, impotence in males • Nervous system – Emotional lability, irritability; • Tremor of the body (symptom of «telegraph post») especially nails of hands (Mary symptom).
Metabolism – subfebrile body temperature, skin is warm • Low body weight. • Ostheoporosis. • Skin is warm and moist, mild, velvet-like; • Pretibial myxedema • Thyroid gland is enlarged, of solid-elastic consistency, systolic murmur above it • Sex glands – mastopathy, gynecomastia
Ophthalmopathy • Exophthalmos* Dalrimpl’s sign (wide eye slits)* Graefe’s sign(white space above cornea if a patient changes point of view from up to down)* Mebiussign (convergention disorders)* Elinek’ssign (eyelids hyperpigmentation)* Stellwag’ssign (rareblinking)* Rosenbach’ssign (tremor of closed eyelids)* Kocher’s sign – exposure of the sclera between the lower edge of the upper eyelid and the upper edge of the iris when the eyes are fixed on the upwardly moved object
Laboratory and instrumental examination • ECG: synus tachicardia, extrasystoly, paroxysmal tachycardia, atrial fibrillation; • Ultrasound examination of a heart: high heart output; • Rogr - cardiomegaly • Metabolism – Increased serum Ca, excretion of Ca with urine • Digestive tract – Changes of indexes of liver function
Ocular symptoms Grefe’s sign
Degrees of severity of thyrotoxicosis Mild Heart rate - less than 100 b/min Body mass defficiensy - less than 10 % Work capacity - preserved or slightly limited Moderate Heart rate - 100 - 120 b/min Body mass defficiensy - 10 - 20 % Changes of other organs and systems - ophthalmopathy Work capacity - decreased Severe Heart rate - more than 120 b/min,atrial fibrillation Body mass defficiensy - more than 20 % Changes of other organs and systems - ophthalmopathy; dystrophy of parenchimal organs Work capacity - lost.
Diagnostics of DTG Anamnesis Provoking factors Clinical pattern Signs of thyrotoxicosis and diffuse enlargement of thyroid gland Laboratory tests 1) Common and free Т3 і Т4are increased; 2) Increased level of common Т3and normal Т4 (Т3 – thyrotoxicosis) 3) Decreased level of thyrotrophic hormone (TTH) 4) Increased consumption of radioactive iodinumJ131with thyroid gland 5) High level of antibodies to TTH receptors
Instrumental diagnostics • Ultrasound examination of thyroid gland (enlargement and diffuse decreased density); 2) Scintigraphy (insuspiction on retrosternal goitre and in nodal goitre) 3) Puncture biopsy of thyroid gland is executed for diagnostics of all nodal formations in the gland
Laboratory and instrumental examination • ECG: synus tachicardia, extrasystoly, paroxysmal tachycardia, atrial fibrillation; • Ultrasound examination of a heart: high heart output; • Rogr - cardiomegaly • Metabolism – Increased serum Ca, excretion of Ca with urine • Digestive tract – Changes of indexes of liver function
Treatment Antithyroid preparations (propilthiouracil, tiamazol (merkasolil) within 1-2 years Mercasolil (5 mg) – 30-60 mg per os, gradually decrease dosage till 5-15 mg. Beta-adrenobloquers (metoprolol 50-200 mg/d, bisoprolol 5-10 mg/d, propranolol 80-120 mg/d
Surgical treatment Indications Large goitre (over 45 cm3); Compresstion or displacement of trachea, esophagus or large vessels; Retrosternal goitre; Severe thyrotoxicosis with atrial fibrillation; No stable effect of medicamentous treatment. Intolerance of antithyreoid drugs, allergy; Nodal goitre with thyrotoxicosis.
Thyrotoxic crisis Provokingfactors Trauma or rude palpation of thyroid gland; Operation on thyroid glandor usage of J131 without previous medicamentous correction; Any operative treatment in persons with hidden and unrecognized thyrotoxicosis; Inflammatory and infectious diseases; Abrupt stop of antithyroid drug therapy; overheating; Physical and psychic trauma; Pregnancy and delivery.
Clinical manifestation Acute beginning; Nervous excitation or psychosis, fear of death; Skin is hot and moist, chande of profound sweating on skin dryness, face is hyperemud, cianosis of limbs, tongue and lips are dry. Muscular weakness, adynamia, pareses; Tachicardia, atrial fibrillation, elevation of BP with its following sudden dropacute left entricular failure; Nausea, vomiting, diarrhoea Lab tests Anemia, leukocitosis, decreased hematocrit; elevated Т3and Т4
Treatment Inhibition of production and secretion of thyreoid hormpones; Inhibition of nervous system irritation; Restoration of adrenal glands function; Correction of cardiovascular disorders; Normalization of voter and salt metabolism acid-alkaline balance; Treatment of hypoxia, hypertermia
1. Complete physical and emotional rest. Mercasolil 20-30 mg per os. 2.Hydrocortison 200-400 мг (prednisolon 3-5 мг/кг), 0,05 % strophanthin 0,5 mli/v. 3. Anaprilin 80 mg per os. 4. Reserpin 0,5 mg per os. 5. In nervous excitation – droperidol 2,5 mg. 6. Permanent oxygen therapy, applictaion of cold. 7. In low BP – cordiamin 2 ml subcutaneously.
Hypothyreosis A disease caused by prolobged permanent thyroid hormones deficiency with following decrease of metabolism and functional disorders in different organs and systems
Epidemiology Spreadingin population 0,2 – 1 %; Among newborns 0,025 % (1 : 4000); People over 65 years – 2 – 4 %. Subclinical and primary hypothyreosis is observed in 7-10 % femalesand 2 – 3 % males.
Ethiology of congenital hypothyreosis Primary: 1) Abnormal thyroid gland development – dysgenesia; 2) Disorders of зу Т3 і Т4 syntesis; 3) Defect of TTH receptors; 4) Iodinum defficiency (endemic cretinism) Secondary: Congenital defects of hypophisis – isolated ТТГ defficiency Tertiary: Congenital defects of hypothalamus Perypheral: resistanse to thyroid hormons
Acquired hypothyreosis Primary: 1) strumectomia; 2) X-ray rtherapy of treatment with radioactive iodinum; 3) medicamentous-induced (зокрема, imidazol derivtives, litium preparation,iodinum preparations, beta-bloquers, interferon, interleukin-2); 4) authoimmune thyreoiditis, infectious affections of the gland (tuberculosis, scleroderma etc.); 5) trauma, hemorrhage, tumor; 6) Iodinum deficiency
Secondary 1) Brain commotion; 2) Tumors and metastases; 3) Brain hemorrage, thrombembolism, atherosclerosis; 4) Inflammations ( authoimmune and infectious); 5) Chemical intoxications including drugs (reserpin, parlodel, apomorphin affect hypophysis, serotonin containing drugs – affect ypothalamus)Perypheral: Inactivation of circulationg Т3, Т4, ТТH, resistance of receptors