Download
1 / 1
10 likes | 107 Views
Correlation of Hand-Foot Skin Reaction (HFS) with Treatment Efficacy in Pancreatic Cancer (PC) Patients (pts) Treated with Gemcitabine/Capecitabine plus Erlotinib: A Subgroup Analysis from the AIO-PK0104 Randomized, Cross-Over Phase III Trial in Advanced PC. #4023.

E N D
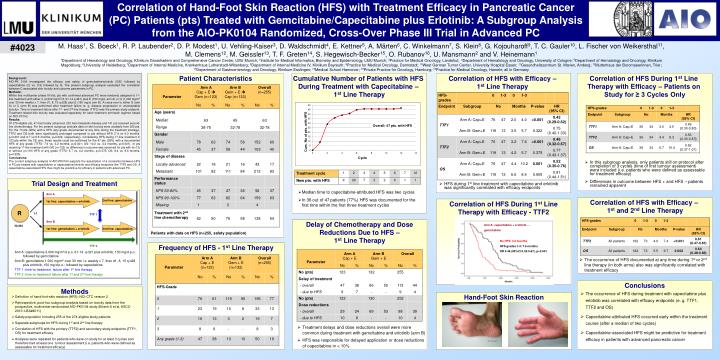
Correlation of Hand-Foot Skin Reaction (HFS) with Treatment Efficacy in Pancreatic Cancer (PC) Patients (pts) Treated with Gemcitabine/Capecitabine plus Erlotinib: A Subgroup Analysis from the AIO-PK0104 Randomized, Cross-Over Phase III Trial in Advanced PC #4023 M. Haas1, S. Boeck1, R. P. Laubender2, D. P. Modest1, U. Vehling-Kaiser3, D. Waldschmidt4, E. Kettner5, A. Märten6, C. Winkelmann7, S. Klein8, G. Kojouharoff9, T. C. Gauler10, L. Fischer von Weikersthal11, M. Clemens12, M. Geissler13, T. F. Greten14, S. Hegewisch-Becker15, O. Rubanov16, U. Mansmann2 and V. Heinemann1 1Department of Hematology and Oncology, Klinikum Grosshadern and Comprehensive Cancer Center, LMU Munich; 2Institute for Medical Informatics, Biometry and Epidemiology, LMU Munich;3Practice for Medical Oncology, Landshut; 4Department of Hematology and Oncology, University of Cologne; 5Department of Hematology and Oncology, Klinikum Magdeburg; 6University of Heidelberg; 7Department of Internal Medicine, Krankenhaus Lutherstadt-Wittenberg; 8Department of Internal Medicine IV, Klinikum Bayreuth; 9Practice for Medical Oncology, Darmstadt; 10West German Tumor Center, University Hospital Essen; 11Gesundheitszentrum St. Marien, Amberg; 12Mutterhaus der Boromaeerinnen, Trier; 13Department of Gastroenterology and Oncology, Klinikum Esslingen; 14Medical School Hannover; 15Private Practice for Oncology, Hamburg; 16Practice for Medical Oncology, Hameln; all in Germany Patient Characteristics Cumulative Number of Patients with HFS During Treatment with Capecitabine – 1st Line Therapy Correlation of HFS with Efficacy – 1st Line Therapy Correlation of HFS During 1st Line Therapy with Efficacy – Patients on Study for ≥ 3 Cycles Only Background: AIO-PK 0104 investigated the efficacy and safety of gemcitabine/erlotinib (G/E) followed by capecitabine (C) vs. C/E followed by G. The present subgroup analysis evaluated the correlation between C-associated skin toxicity and outcome parameters in PC. Methods: Within this multicenter phase III trial, pts with confirmed advanced PC were randomly assigned to 1st-line treatment with either C (2,000 mg/m2/d, d1-14 q d21) plus E (150 mg/d, arm A) or G (1,000 mg/m2 over 30 min weekly x 7, then d1, 8, 15 q d28) plus E (150 mg/d, arm B). A cross-over to either G (arm A) or C (arm B) was performed after treatment failure (e. g. disease progression or unacceptable toxicity). Time to treatment failure after 1st- and 2nd-line therapy (TTF2) was the primary study endpoint. Treatment-related skin toxicity was evaluated separately for each treatment arm/each regimen based on NCI-CTCv2. Results: Of 279 eligible pts, 47 had locally advanced, 232 had metastatic disease and 141 pts received second-line chemotherapy. For the present subgroup analysis data on skin toxicity were available from 255 pts. For the 73 pts (29%) with a HFS (any grade documented at any time during the treatment strategy), TTF2 and OS both were significantly prolonged compared to pts without HFS (7.4 vs 4.0 months, p<0.001 and 9.7 vs 5.5 months, p=0.002, respectively). Considering HFS during 1st-line treatment in 123 pts within the CE arm, these results could be confirmed for the 47 pts (38%) with a documented HFS of any grade (TTF2: 7.6 vs. 3.2 months, p<0.001; OS: 10.2 vs. 4.4 months, p=0.001). In pts receiving 1st-line treatment with G/E (n=132) no difference in outcome was observed for pts with (n=13) or without (n=119) HFS of any grade (TTF2: 5.7 vs. 4.2 months, p=0.375; OS: 8.4 vs. 6.6 months, p=0.505). Conclusions: The current subgroup analysis of AIO-PK0104 supports the assumption of a correlation between HFS in PC pts treated with capecitabine or capecitabine/erlotinib and efficacy endpoints like TTF2 and OS. A capecitabine-associated HFS thus might be predictive for efficacy in patients with advanced PC. Overall: 47 pts. with HFS • In this subgroup analysis, only patients still on protocol after completion of 3 cycles (time of first tumour assessment) were included (i.e. patients who were defined as assessable for treatment efficacy) • Differences in outcome between HFS + and HFS – patients remained apparent Trial Design and Treatment • HFS during 1st line treatment with capecitabine and erlotinib was significantly correlated with efficacy endpoints • Median time to capecitabine-attributed HFS was two cycles • In 36 out of 47 patients (77%) HFS was documented for the first time within the first three treatment cycles Arm A Correlation of HFS with Efficacy – 1st and 2nd Line Therapy 2nd line: gemcitabine 1st line: capecitabine + erlotinib Correlation of HFS During 1st Line Therapy with Efficacy - TTF2 R 1:1 TTF 1 Arm B Delay of Chemotherapy and Dose Reductions Due to HFS – 1st Line Therapy Arm A: capecitabine + erlotinib → gemcitabine N=281 1st line: gemcitabine + erlotinib 2nd line: capecitabine Patients with data on HFS (n=255, safety population) No HFS: 3.2 months HFS grades 1-3: 7.6 months HR 0.46 (95%CI 0.32-0.67), p<0.001 Frequency of HFS - 1st Line Therapy TTF 2 Arm A: capecitabine 2.000 mg/m2/d p.o. d1-14, q d21 plus erlotinib, 150 mg/d p.o.; followed by gemcitabine Arm B: gemcitabine 1.000 mg/m2 over 30 min i.v. weekly x 7, then d1, 8, 15 q d28 plus erlotinib, 150 mg/d p.o.; followed by capecitabine TTF 1: time-to-treatment failure after 1st line therapy TTF 2: time-to-treatment failure after 1st and 2nd line therapy • The occurrence of HFS documented at any time during 1st or 2nd line therapy (in both arms) also was significantly correlated with treatment efficacy Conclusions Methods • The occurrence of HFS during treatment with capecitabine plus erlotinib was correlated with efficacy endpoints (e. g. TTF1, TTF2 and OS) • Capecitabine-attributed HFS occurred early within the treatment course (after a median of two cycles) • Capecitabine-associated HFS might be predictive for treatment efficacy in patients with advanced pancreatic cancer Hand-Foot Skin Reaction • Definition of hand-foot-skin reaction (HFS): NCI-CTC version 2 • Retrospective, post-hoc subgroup analysis based on toxicity data from the prospective, multicenter randomized AIO-PK0104 study (Boeck S et al, ASCO 2010: LBA#4011) • Safety population including 255 of the 274 eligible study patients • Separate subgroups for HFS during 1st and 2nd line therapy • Correlation of HFS with the primary (TTF2) and secondary study endpoints (TTF1, OS) for treatment efficacy • Analyses were repeated for patients who were on study for at least 3 cycles and therefore had at least one tumour assessment (i.e. patients who were defined as assessable for treatment efficacy) • Treatment delays and dose reductions overall were more common during treatment with gemcitabine and erlotinib (arm B) • HFS was responsible for delayed application or dose reductions of capecitabine in < 10%






















