Download
1 / 13
130 likes | 147 Views
Learn about the differences between type 1 and type 2 diabetes, their symptoms, potential complications, diagnosis methods, emergencies like ketoacidosis and hypoglycemia, medical management strategies, and how to address diabetes in dental care settings.

E N D
Diabetes Claire Nowlan Nov 28, 2003
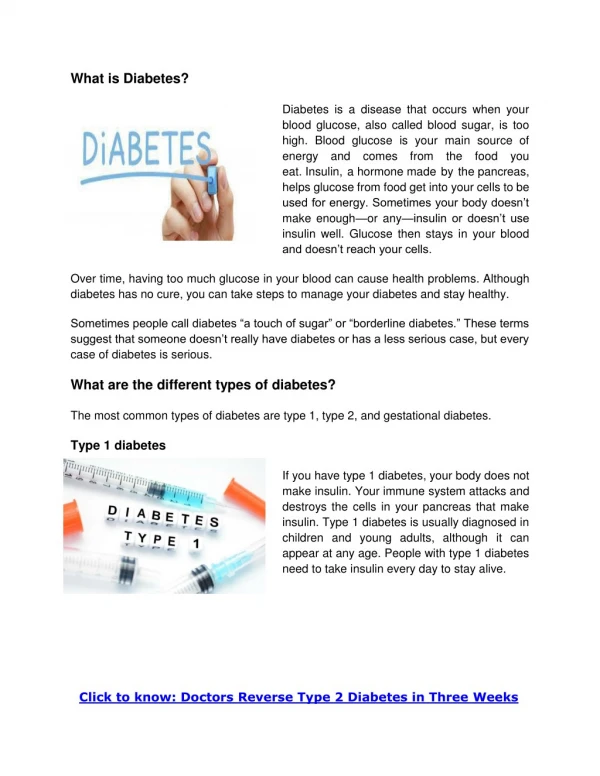
Type 1 10% of diabetics Age of onset – young Severe Requires insulin Normal build Little genetic component Type 2 90% of diabetics Age of onset – 40+ Mild May require insulin, usually hypoglycemics Obese Strong genetic component Comparison of type 1 and 2 diabetes
Pathophysiology • Type 1 diabetes – beta cells are destroyed, eventually no insulin is produced • Type 2 diabetes – insulin secretion is reduced, target cells become relatively insulin resistant
The Pancreas • Main role is to excrete digestive enzymes • Islets of Langerhans contain alpha cells which excrete glucagon, and beta cells which excrete insulin • Glucose stimulates insulin secretion from beta-cells • Insulin binds with cells surface receptors to allow glucose transport into the cell • Glucagon mobilizes glucose to be released from the liver
Symptoms of diabetes • Polydipsia (increased drinking) • Polyuria (increased urination) • Weight loss • Weakness • Increased infections • Blurred vision
Complications • Macrovascular • Stroke • MI • Ulcers • Amputation • Microvascular • Retinopathy - blindness • Nephropathy – renal failure • Neuropathy – numbness, tingling, pain , sensory deficits, and autonomic involvement • Infections
Lab tests - diagnosis • Random glucose • >11.0 mmol/L + symptoms • Fasting glucose • >6.9 mmol/L • Hb A1c • A long term measure of diabetic control • > 8%
Emergencies • Ketoacidosis • In type 1 patients only • Marked hyperglycemia (high serum glucose) causes osmotic diuresis • Patient loses excess water, Na, K, and ketones released from the liver cause an acidosis • Precipitated by an infection, insulin error or omission, or occurs in a previously undiagnosed patient • Treated with insulin, fluid replacement, K replacement • Type 2 diabetics can have a much less serious variant of this called Hyperglycemic hyperosmolar nonketotic state
Emergencies • Hypoglycemia • May occur with an overdose of insulin/oral medication or a missed meal • Only some medications cause hypoglycemia – Glyburide, Glicazide, Chlorpropamide • Patient gets diaphoretic, weak, shaky, palpitations, difficulty thinking, vision changes and may lose consciousness • Patient needs glucose – a glass of juice, a candy, or if comatose, IV 50% glucose solution, IM glucagon, glucose gel • Some patients are totally unaware of their hypoglycemia until they lose consciousness
Medical management • The tighter the control, the fewer complications– BUT – the more risk of getting hypoglycemic • IDEAL management • Fasting glucose 4.0 – 7.0 mmol/L • 1-2 hour postmeal 5.0 – 11.0 mmol/L • Type 1 diabetes – insulin tx– usual starting dose about 20 units/day (testing 2-5 x/day) • Type 2 diabetes – oral hypoglycemics +/- insulin (testing 1-2x/day) - diet only (testing 2x/month) • Infection, stress, pregnancy, surgery will all disturb control
Dental management • Assess control/severity • What medications are you taking (or diet only) • Type 1 vs Type 2 • When were they first diagnosed • How often do they measure their glucose • What are their usual measurements • Frequency of hypoglycemic reactions (can they feel them coming on?) • How much insulin do they use • When did they last see their doctor
Your biggest worries: • Hypoglycemia during a procedure • Oral surgeries that will prevent the patients from getting their usual caloric requirements • Brittle diabetics (extreme fluctuations of hypo/hyperglycemia) – usually occurs after years of high dose insulin therapy • Acute oral infections that precipitate hyperglycemia • Be more aggressive with antibiotics in patients with high sugars
Oral complications • Xerostomia • Infections – especially candidiasis • Increases caries • “Burning mouth syndrome” • So – test for diabetes in suspicious patients