Download
1 / 10
100 likes | 263 Views
Case #1. Patient: HC, 61-year old, Male. Case #1. Case #2. Patient: JW, 51-year old, Airline Pilot. Case #2. Case #3. Patient: 27-year old, Female. Case #3. Discussion.

E N D
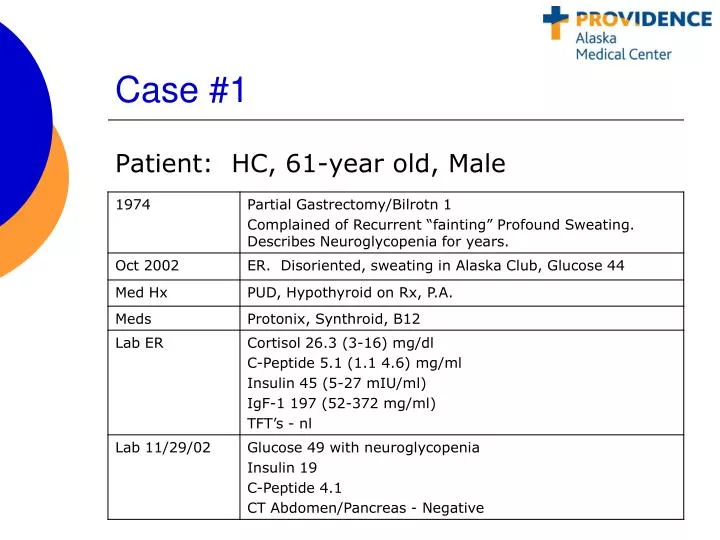
Case #1 Patient: HC, 61-year old, Male
Case #2 Patient: JW, 51-year old, Airline Pilot
Case #3 Patient: 27-year old, Female
Discussion • Severe postprandial hypoglycemia with hyper insulinemia has recently been described as a complication of Roux-en-Y gastric bypass. • The pathophysiology leading to this is far from clear. • It is poorly responsive to nutritional or medical therapy and may require partial pancreatectomy for treatment. • Historically; variability sized islets, diffuse islet hyperplasia and increased Beta-cell volume.
Discussion • Hypothesis that long term stimulation of Beta-cell growth and activity by gut hormones such as the incretin hormone GLP-1 could be a contributing factor. • Goldfine, et.al (JCEM) showed an increase in GLP-1 response to meal intake up to at least 3 years after RYGB. An exaggerated GLP-1 response has been observed after other types of surgeries expediting the contact between nutrients and the hindgut. • This response has not been observed following purely restrictive procedures such as adjustable gastric banding.
Discussion • Vidal, et. Al (JCEM, March 2009) failed to support the hypothesis that the sustained increase in the postprandial GLP-1 response results in inappropriate insulin secretion relativetotheprevailinginsulinsensitivity. • It has been shown that Beta cells have a tight control system to limit the effects of growth and differentiation by GLP-1. Also, the beta cells may express negative regulators of key signaling pathways involved in cell proliferation. It is possible that symptomatic hypoglycemicpatients may have defects in these regulatory pathways allowing for more insulin secretion to occur.
Discussion • Perhaps, by slowing carbohydrate absorption with alpha glucosidase inhibition, hypoglycemia can be mitigated.










