Download
1 / 25
330 likes | 924 Views
Liver Transplant Evaluation: The Process. Ris ё Stribling , MD Medical Director of Liver Transplant St Luke’s Medical Center Associate Professor of Surgery Baylor College of Medicine. Liver Transplant Clinical Indications. Decompensated cirrhosis- all causes

E N D
Liver Transplant Evaluation: The Process RisёStribling, MD Medical Director of Liver Transplant St Luke’s Medical Center Associate Professor of Surgery Baylor College of Medicine
Liver TransplantClinical Indications • Decompensated cirrhosis- all causes • Hepatocellular carcinoma- defined criteria • Acute liver failure • Hepatopulmonary Syndrome • Portopulmonary Hypertension • Metabolic disorders
LIVER TRANSPLANT – INDICATIONS AND CONTRAINDICATIONS Liver Transplant Contraindications • Extrahepatic malignancy • Active infection • Active substance abuse • Cholangiocarcinoma-relative • Significant non-hepatic co-morbidity • Significant portal/SMV thrombosis
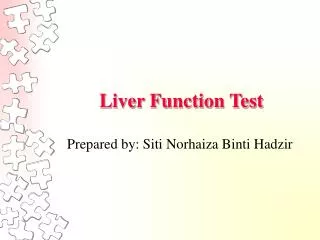
Cirrhosis Histopathologic Result of Chronic Liver Diseases Normal Liver Cirrhosis
DEFINITION OF CIRRHOSIS Cirrhosis • End stage of any chronic liver disease • Characterized histologically by regenerative nodules surrounded by fibrous tissue • Clinically there are two types of cirrhosis: • Compensated • Decompensated
NATURAL HISTORY OF CHRONIC LIVER DISEASE Development of complications: • Variceal hemorrhage • Ascites • Encephalopathy • Jaundice Natural History of Chronic Liver Disease Chronic liver disease Compensated cirrhosis Decompensated cirrhosis Death
NATURAL HISTORY OF CIRRHOSIS Development of Complications in Compensated Cirrhosis 100 80 Ascites 60 Probability of developing event Jaundice Encephalopathy 40 GI hemorrhage 20 0 0 20 40 60 80 100 120 160 140 Months Gines et. al., Hepatology 1987; 7:122
SURVIVAL TIMES IN CIRRHOSIS Decompensation Shortens Survival 100 Median survival ~ 9 years 80 All patients with cirrhosis 60 Probability of survival 40 Decompensated cirrhosis 20 Median survival ~ 1.6 years 0 0 20 40 60 80 100 120 140 160 180 Months Gines et. al., Hepatology 1987;7:122
Cirrhosis and Decompensation • Compensated cirrhosis patients may be followed for years but once decompensation occurs, liver transplant referral should be done promptly.
Liver Transplant Referral • The initial step of the liver transplant referral process is financial clearance. This step requires the designated center to attain financial clearance to begin the evaluation process. • It is important to note that neither the patient or the physicians may obtain this clearance. • This step may take any where from a few hours up to a few weeks depending on the insurance company.
The Liver Transplant Evaluation Process • Once financial clearance is obtained, the liver transplant coordinator will begin communication with the patient. • The transplant coordinator is there to review the records, place the orders for the tests, imaging, and consultations needed. • This evaluation is usually completed over several days
The Liver Transplant Evaluation Process • The patient will have consultations with the following team members during the evaluation: • Transplant Financial Counselor • Liver Transplant Surgeon • Transplant Hepatologist • Transplant Social Worker • Transplant Dietician • Transplant Coordinator • Transplant Cardiologist- as needed • Other consultants are based on medical indications such as Anesthesia, Pulmonary, Nephrology, Hematolgy/Oncology
Social Worker Evaluation • Full assessment of the social support for a patient • Development of a suitable 24 hour care plan • Evaluation of patient’s financial status to determine if the out of pocket expenses are within the patient’s financial means • Assessment of the home including pets: reptiles, birds, cats, chicks/ducklings, exotic pets such as monkeys • Alcohol and substance use history including any co-existing psychiatric issues • Recommendations for psychiatric evaluation of substance abuse treatment/relapse prevention • Functional status of the patient • Assess the level of commitment to the transplant process, follow up and compliance • Assess for the medical power of attorney, directives to physicians
Medical Review Board • The case is then taken to a Medical Review Board • It is at this time that the case is fully reviewed with presentations by the primary team members including surgery, hepatology, social worker, dietician, financial counselor. • Recommendations from the MRB are made on the needed labs, imaging, and additional consultations are made at this stage
Liver Transplant Listing • Once full clearance is obtained from the medical review board, the patient is then listed for liver transplant using the MELD score determination
MELDModel of End Stage Liver Disease • Formula based on bilirubin, INR, creatinine – no subjective component • Predicts mortality at 90 days • Adopted for liver allocation in Feb 2002 • Sickest get transplanted first • Avoids certain problems with CTP • Accurate in about 80% of patients – requires certain exceptions
MELD AND SURVIVAL ON TRANSPLANT WAITING LIST MELD and Survival on Transplant Waiting List 100 92.3% < 15 80 90.7% 15-20 60 Probability of survival (%) 66.0% 20-29 40 33.8% > 30 20 0 12 0 2 4 6 8 10 Months from listing
Share 35 Program • This is the newest organ allocation policy. • This program requires regional sharing of organs in all patients whose MELD is greater than 35. • This program has made a dramatic difference in our abilities to get organs for the sickest patients.
UNOS REGIONS United Network for Organ Sharing (UNOS) Regions 1 7 6 9 2 10 8 11 5 3 4
SUMMARY • Cirrhosis decompensation such as ascites, encephalopathy, GIB, jaundice should all prompt referral to a liver transplant center • Liver transplant assessment is commonly done by the transplant hepatologist with a full evaluation recommended once the MELD score is >15 or if there is a suspected HCC which is within the specified criteria • The liver transplant referral process may take days to weeks to complete in the outpatient setting. • Urgent inpatient evaluations can be done in 1-2 days. • Patients are listed in UNOS based on their MELD scores
Question 1 Which of the following is the most common cause of cirrhosis prompting liver transplant in the U.S.? 1. Alcohol abuse 2. Hepatitis B 3. Hepatitis C 4. Acute Tylenol overdose
Question 2 At what time should a liver transplant evaluation be considered? 1. When the patient first receives the diagnosis of cirrhosis 2. Once the patient deteriorates and is in the ICU 3. When there is evidence of decompensation of the cirrhosis 4. When the crash cart arrives to the bedside
Question 3 When following cirrhosis patients, calculation of the MELD score helps to assess the time at which liver transplant referral should be done. What MELD score has been shown to be the time for transplant referral? 1. MELD < 15 2. MELD >25 3. MELD >15