Download
1 / 87
1.09k likes | 3.02k Views
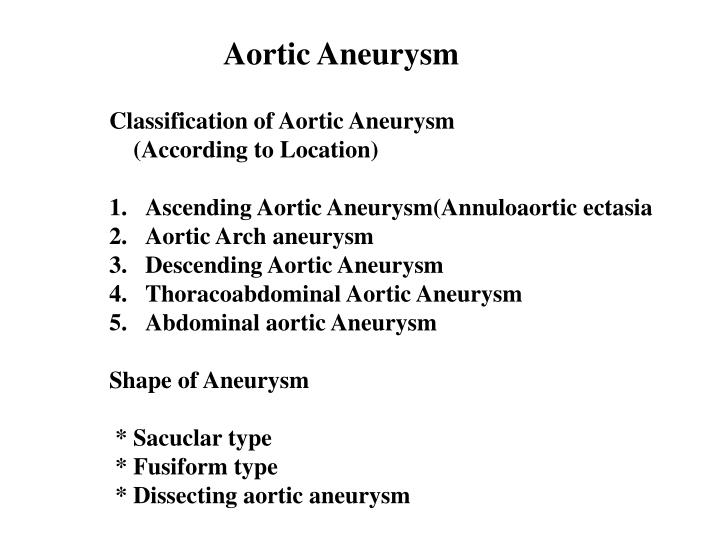
Aortic Aneurysm. Classification of Aortic Aneurysm (According to Location) Ascending Aortic Aneurysm(Annuloaortic ectasia Aortic Arch aneurysm Descending Aortic Aneurysm Thoracoabdominal Aortic Aneurysm Abdominal aortic Aneurysm Shape of Aneurysm * Sacuclar type * Fusiform type

E N D
Aortic Aneurysm • Classification of Aortic Aneurysm • (According to Location) • Ascending Aortic Aneurysm(Annuloaortic ectasia • Aortic Arch aneurysm • Descending Aortic Aneurysm • Thoracoabdominal Aortic Aneurysm • Abdominal aortic Aneurysm • Shape of Aneurysm • * Sacuclar type • * Fusiform type • * Dissecting aortic aneurysm
Etiologic Classification • Congenital aneurysm • Acquired aneurysm • * Atherosclerotic aneurysm • * Traumatic aneurysm • * Syphilitic aneurysm • * Mycotic aneurysm • * Dissecting aneurysm
Thoracic Aortic Aneurysm Indication for operation Ascending Aneurysm * Progressive enlargement of the aneurysm(5-6 cm) * Signs and symptomes of aortic valvular regurgitation (Bentall procedure) Transverse Aneurysm * Symptoms(dyspnea,stridor,hoarseness,hemoptysis,cough, and chest pain) * In the fusiform medial degenerative type,diameter > 5cm Descending Aneurysm * All symptomatic patients * diameter is twice that of the normal aorta(around 6 cm) * Acute enlargement
Thoracoabdominal Aortic Aneurysm Crawford Classification Type I : Aneurysms involve all or most of the descending thoracic aorta and suprarenal abdominal aorta Type II : Aneurysms involve all or most of the descending thoracic aorta and all or most of the abdominal aorta Type III :Aneurysms involve distal half or less of the descending thoracic aorta and varying segments of the abdominal aorta Type IV: Aneurysms involve all or most of the abdominal aorta
Clinical Symptomes and Sign of the Dissecting Aortic Aneurysm
Aortic Dissection Splitting of the medial layer of the Aortic wall,associated with intimal Flap---Inlet—develope false and true lumen
Aortic Dissections Classification Stanford Classification Type A: Dissection involving the ascending aorta Type B: Dissection involving the descending aorta DeBakey Classification Type I: An intimal tear,commonly located in the anterior ascending aorta and progressing through the arch into the descending aorta,whole abdominal aorta Type II: Dissections are confied to the ascending aorta Type III: Involving only the descending aorta(Type IIIa: ,Restricted to the thoracic aorta. TypeIIIb: involving in abdominal aorta and extending distally)
Clinical Presentation and Diagnosis Hemodynamic State *Sudden death *Hypovolemic shock *Cardiogenic shock(acute AR 35-60%) Symptomes and Signs * Sudden severe pain and feeling of impending death (Often interscapular pain,precordial and radiate into neck or arm) * Painless * Ischemic sypmtomes of occlusion of a major vessels. Diagnosis 1. Chest x-ray 2. Ecchocardiography 3. CT scan 4. Aortography or MRA
Surgical Indication of Dissecting aortic Aneurysm Type A--- Indication is made once diagnosis has been confirmed and the patient can be stabilized with drugs therapy Type B--- 1. Progress of dissection process 2. Impending rupture of dissecting aneurysm 3. Poor control of BP and pain persists or progesses to the abdomen under intensive medication 4.Organ or limb ischemia,neurologic sign with paresis or paralysis
The Major Risk Factors for Aortic Reconstruction * Adequate cerebral protection * Bleeding coagulopathy * Protection of the ischemic myocardium
Advance Improvement in Aortic Reconstruction * Graft technique * Anastomotic technique * Use of echocardiography * Improved hemotology * Myocarial and cerebral protection
CEREBRAL PROTECTION 1.Profound Deep Hypothemia Central Temperature :16-18 *C 2. Deep Hypothemia Central Temperature: 18-20 *C 3. Moderate Hypothemia Central Temperature: 26-28 *C + Separate Carotid Blood Perfusion 4. Deep or Moderate Hypothemia Central Temperature: 20-23 *C + Retrograde SVC Blood Perfusion
Rupture Risk of AAA Rupture rate per year Less than 4 cm diameter 0% 4-5 cm diameter 0.5-5% 5-6 cm diameter 3-15% 6-7 cm diameter 10-20% 7-8 cm diameter 20-40% More than 8 cm diameter 30-50%
The Confirm Diagnosis for A.A.A. • Regularly physical check up • Ultrasound • CT scan 3mm-5mm interval, 3-D reconstruction • Angiographies • MRI
Symptoms for A.A.A. • Usually a symptomatic • Incidental finding • Palpable mass in mid abdomen • Back pain • Abdominal fullness, abdominal pain
Postoperative Complications of Aneurysmectomy of the AAA • Bleeding • Infection • Rupture • False Aneurysm • Change in Sexual Function • Spinal Ischemia
Ischemic Colitis Following Aortic Reconstruction • Ligation of IMA(improper) • Loss of IMA-hypogastric blood flow • Rupture aneurysm • Perioperation hypotension-hypoperfusion • Manipulative trauma • Inadequate collateral development • IMA SMA flow in meandering mesenteric
Criteria for Endovascular Treatment • Maximum angulation of the neck <60 degree • Grade I,IIA,IIB,infrarenal neck length >1.5 cm • Proximal aortic neck diameter <28 mm • Common iliac diameter < 20 mm • No thrombus lined or calcified aortic neck
Indications for Endovascular Treatment of Aortic Aneurysm • Asymptomatic AAA more then 5 cm in diameter • All symptomatic or rupture aneurysm • High risk patient and unfit for conventional open repair • Older patients ,even an AAA less than 4 cm in diameter
Contra Indication for Endovascular Treatment • Short neck <10mm • Wide angle >75° • Conical neck 3mm/10mm • Calcified or thrombus surround the neck • Torturous iliac artery>90° • Calcified iliac artery • Iliac aneurysm • Short iliac artery
Potential Adverse Events of Endovascular Repair • Death • Emboli and subsequent tissue damage or loss • Perforation of aorta • Hypotension • Pseudoaneurysm at the vascular access site • Infection and pain • Contrast reaction • Vessel damage • Iliac stenosis • Myocardial infarction • Bowel ischemia • Claudication • Renal complications
The Procedures and Tips for Placing Endovascular Stent Graft
Follow up for the Endovascular Stent Graft Procedure • Graft migration • Endoleak I. Neck,iliac II. Retrograde flow III. Device failure IV. Porosity • Kinking of graft • Size of the sac
Other Complications • Injury to artery • Embolization • * Postimplant syndrome • Graft limb thrombosis • Groin wound infection • Conversion to open repair • Aortic rupture • Endograft migration obstruction • Persistent endoleak • Endograft infectin
Future Trend for the Endovascular Procedure • Overcome present difficulties • Ruptured A.A.A. • Aortic dissection • Thoracic aneurysm or aneurysm in other sites
Surgical treatment of the Ischemic heart disease • Clinical symptome , diagnosis and treatment of aortic dissection • Surgical treatment of the aortic disease • Pathophysiology of pulmonary hypertension • Clinical symptoms and signs of pulmonary embolism • Management of pulmonary embolism • Clinical symptoms,signs and diagnosis of peripheral vascular disease • Medical and surgical treatment of the peripheral vascular disease
Surgical Treatment of the Ischemic Heart Disease
Major Clinic Presentations of Ischemic Heart Disease • Stable angina pectoris • Unstable angina pectoris • Acute myocardial infarction • Less commnon presentations: • * Silent ischemia • * Sudden death • * Arrhythmia • * Congestive heart failure • * Papillary muscle dysfunction with MR
Risk factore for operative morbidity and mortality in CABG surgery • Age above 70(1.5-2 fold increase in mortality rate) • Left ventricular dysfunction(2-3 fold increase) • Female gender(1.2-1.5 fold increase) • Previous CABG operation(2.5-3.5 fold increase) • Diabetes mellitus(1.2-1.5 fold increase) • Peripheral vascular disease(1.2-1.5 fold increase) • Chronic renal failure(1.5-1.9 fold increase) Main operative morbidity * Cerebrovascular accident (2%) * MI (3%) * Mediastinitis(1%)
Conduits for CABG • Greater saphenous vein • Lesser saphenous vein • Left and right internal mammary arteries • Radial artery • Right gastroepiploic artery • Inferior epigastric artery
CONDUITS FOR BYPASS GRAFTING * Saphenous Vein Grafts * Internal Mammary Artery Grafts Alternate Conduits * Gastroepiploic Artery * Inferior Epigastric Artery * Radial Artery * Cryopreserved Homograft Veins
Surgical Indications for coronary artery bypass grafting • Unstable angina • Left Main CAD • Symptomatic tree vessel(TVD) with Failure of medical therapy • depressed LV function • Postinfarction angina • Acute myocardial infarction with cardiogenic shock • Failure PTCA or stent • Reoperation for recurrent symptomes • Congenital anomalies of coronary arteries • Kawasaki’s disease
Indications for insertion of an intraaortic balloon pump (IABP) in acute coronary events • Inadequate response to medical therapy(resistent pain or EKG change) • Failure angioplasty with hemodynamic unstability • Preoperative evidence of significant myocardial injury or hemodynamic instability • Marked ST-T changes during anesthetic induction for CABG
Incremental Risk Factors for Premature Death After CABG * Number of vessels with important stenoses * Preoperative poor left ventricular function * Chronic congestive heart failure * Unstable angina * Emergency surgery for acute infarction with hemodynamic compromise * Older age
Acute Ischemia Medical therapy to stabilize Unstable Stable Mechanical defect Ischemia Functional Cardiac study catheterization VSD MR Free wall Ischemia No ischemia rupture Cardiac catheterization Consider open surgery
Indications for Cardiac Operation in Patients with Acute MI • Mechanical complications after MI(papillary muscle rupture with acute MR,postinfarction ventricular septal defect or free wall rupture,left ventricular aneurysm) • Cardiogenic shock after MI • Evdence of MI extension(continued symptomes,EKG changes,additional elevation of cardiac enzymes) • CABG or PTCA for evolving MI(During the first 4-6 hous after MI), acute complications of PTCA,or stent • Unstable angina with failure of medical management • Severe left main coronary artery stenosis
Postinfaction ventricular septal defect Timing of Operation * Waiting for several weeks--Small minority of patient,the hemodynamic insult is less severe and better tolerated * Prompt operation--Persistence of congestive heart failure with low cardiac output # Shortening the duration of shock by operation early is the only therapeutic solution and yield dramatic results
Postinfaction ventricular septal rupture Survival * Overall hospital mortality of 10-25% Sander RJ ,Skillington et al,Dagget WN et al. (1975-1989 report) Correction of posterior defect 24-32% Closure of anterior defect 12-15%
Postinfaction ventricular septal rupture Preoperative therapy Stabilization of the hemodynamic condition 50-60% present with severe congestive heart failure and a low cardiac output * Reduce the systemic vascular resistance * Maintain cardiac output and arterial pressure * Maintain or improve coronary artery bloodflow
Surgical Treatment of Left Ventricular Aneurysm Incidence and nature history 10-35% aneurysm dilatation of the LV occures in transmural MI Variable motality rates without operation 73% less than 3 years 88% less than 5 years Schlicher et al. 53% at 5 years 88% at 10 years Proudfit et al
Pathophysiology * LV dysfunction * Mural thrombus * Ventricular arrhythmias * Ventricular rupture * Mitral insufficiency
Surgical Treatment of Left Ventricular Aneurysm • Plication of LV Aneurysm • Aneurysmectomy with linea repair of LV aneurysm • Endoventricular patch plasty reconstruction • Dor’s Operation
ENDOVENTRICULAR CIRCULAR PATCH PLASTY FOR SURGICAL TREATMENT OF LARGE LEFT VENTRICULAR WALL ASYNERGIES(LVWA) Definition LV aneurysm or wall motion abnormalities Permanent cardiac failure,NYHA III-IV Clinical criteria Dilated failing ventricle(DFV) or LVWA EF <30%,mean PAP >25 mmHg, LV circumference asynergy >60% LVEDV >250 ml(LDVI >140ml)
B A Dor’s operation for treatment LV aneurysm D C
ENDOVENTRICULAR CIRCULAR PATCH PLASTY FOR SURGICAL TREATMENT OF LARGE LEFT VENTRICULAR WALL ASYNERGIES(LVWA) TENIQUE * CABG before left ventricular reconstruction(LVR) * Left atrial or ventricular approach for repair MR * Crytherapy or subtotal endocardectomy for ventri- cular arrhythmia * Endoventricular circular suture 1-2 cm above sound muscle(put inflated balloon in the ventricular cavity ,diastolic volume of 50-70 ml/m2),cannot be directly suture the revascularied LAD area. * Septal exclusion,folded on the patch.
Coronary Reoperations * Up to 15% of revascularization today * The risk of coronary revascularization is higher than for first operation 3-4 times risk of death 2 times risk of stroke 8 times risk of perioperative MI
Combined Coronary and Carotid Artery Disease * Evaluation of the patients * Etiology of cerebral injury during CABG * Operative strategy