Download
1 / 77
1.13k likes | 2.79k Views
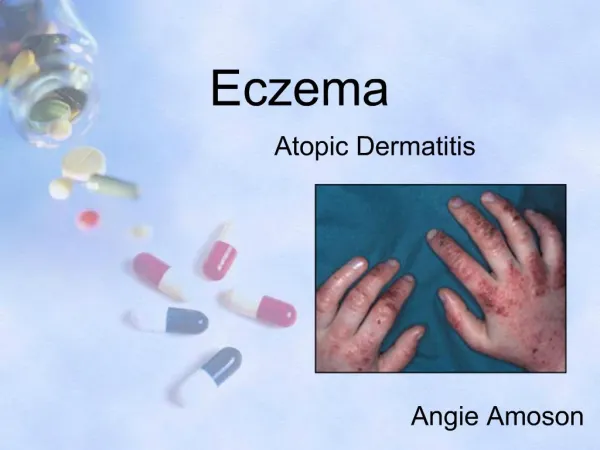
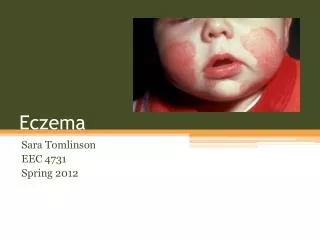
ECZEMA. Definition. Eczema is an inflammatory condition of the skin that is characterized by erythema , papulo -vesicles, oozing & crusting in the acute stages & lichenification in the chronic stages. ' Ekze ', in Greek means “to boil over”.

E N D
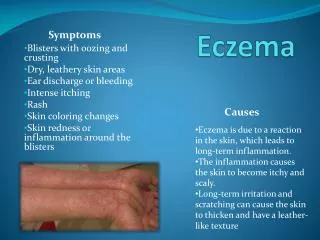
Definition • Eczema is an inflammatory condition of the skin that is characterized by erythema, papulo-vesicles, oozing & crusting in the acute stages & lichenification in the chronic stages. • 'Ekze', in Greek means “to boil over”. • All eczema is dermatitis, but not all dermatitis are eczemas.
The “Itch / Scratch” Cycle The sensation of itch and subsequent scratching is hallmark of most eczemas scratch itch scratch itch
Classification • Irritant dermatitis • Allergic contact dermatitis • Photodermatitis • Dermatophytid • Hand eczema Exogenous eczemas Endogenous eczemas • Atopic dermatitis • Pityriasis alba • Seborrhoeic dermatitis • Discoid eczema • Hand eczema • Asteatotic eczema • Gravitational eczema • Lichen simplex chronicus • Prurigonodularis
Classification • Exogenous eczemas Those related to clearly defined external trigger factors; inherited tendencies may play a part. • Endogenous eczemas Those mediated by internal factors; that is, processes originating within the body. • Some types of eczema are precipitated by both external and internal factors.
Clinical stages • The inflammatory changes of eczema evolve through three stages: • Acute eczematous inflammation • Subacute eczematous inflammation • Chronic eczematous inflammation • The skin changes vary in different stages.
Acute eczematous inflammation Classical clinical features • Intense itching • Intense erythema • Oedema • Papulovesicles • Oozing Examples: Contact dermatitis, Id eruption, Pompholyx
Subacute eczematous inflammation Classical clinical features • Erythema (lesser than in acute stage) • Crusting and scaling • Fissuring • Slight to moderate itching • Stinging and burning sensation Examples: Asteatotic eczema, Atopic dermatitis, Eczematizedtinea
Chronic eczematous inflammation Classical clinical features • Dryness of skin • Excoriation • Fissuring • Lichenification Examples: Lichen Simplex Chronicus, Atopic dermatitis, Nummular eczema
Secondary dissemination Auto-eczematization • Eczema has a characteristic tendency to spread far from its point of origin, known as secondary dissemination or autoeczematization. • Secondary eczema lesions :small, oedematous papules and plaques, grouped papulovesicles. • It subsides, if the primary lesion settles; but it often recurs, if the primary lesion relapses.
Secondary dissemination Mechanisms • Contact with an external allergen • Ingestion or injection of an allergen • Conditioned hyperirritability • Bacterial hypersensitivity
Exogenous Eczemas Contact dermatitis
Irritant dermatitis • Non-immunologic inflammatory reaction of the skin due to an external agent • Varied morphology • Clinical types • Symptomatic (subjective) irritant responses • Chemical burns • Acute irritant contact dermatitis • Chronic irritant contact dermatitis
Chronic irritant dermatitis: common irritants Common irritants • Water and wet work; sweating under occlusion • Household agents: detergents; soaps; shampoos; disinfectants • Industrial cleaning agents: solvents; abrasives • Alkalis, including cement; acids • Cutting oils; organic solvents • Oxidizing agents, including sodium hypochlorite Contd….
Chronic irritant dermatitis: common irritants • Reducing agents, including phenols; aldehydes • Certain plants • Pesticides • Raw food; animal enzymes and secretions • Dessicant powders; dust; soil • Miscellaneous chemicals
Chronic irritant dermatitis: Personsatrisk • Mothers; due to repeated changing of child’s diapers • Housewives • Persons with atopic diathesis • Persons in occupations of : • Hairdressing • Medical, dental, veterinary • Food preparation, catering, fishing • Printing and painting, metal work • Construction
Allergic contact dermatitis • Delayed-type hypersensitivity reaction that occurs upon contact of the skin with an allergen • Inflammatory reaction following absorption of antigen applied to the skin with prior sensitization • Develops within 12 to 48 hours of antigen exposure and persists for 3 to 4 weeks
Allergic contact dermatitis Clinical features • Acute inflammation • Well demarcated patches of erythema, edema, vesicles or bullae. • Linear, erosive and crusted lesions • Chronic inflammation • Lichenification; scaling; or fissures • Clinical features depend on location; duration of contact with allergen • Intensity of the inflammation depends on the degree of sensitivity, concentration of antigen
Allergic contact dermatitis: Patch testing • It is the miniature reproduction of eczema by application of allergens on the intact skin of patients of allergic contact dermatitis. • It should be undertaken for patients in whom the inflammation persists even after the avoidance of the offending agent and the appropriate topical therapy.
Photodermatitis • An eczematous response of skin to sunlight • Distribution typically on the light exposed areas of the skin • Types of reactions to sunlight : • Photo-toxic • Photo-allergic • Eczematous polymorphic light eruptions
Photodermatitis • Systemic/ topical drugs, chemicals, contactants in combination with UVA spectrum induce phototoxic and photoallergic reactions.
Phototoxicreactions: Inducing agents Topical • Perfumes • Dyes • Psoralens • Tars • Plants (lime, celery) Systemic • Psoralen • Tetracycline • Phenothiazine
Photoallergicreactions: Inducing agents Topical • Perfumes (soaps, aftershave) • Sunscreens (PABA) • Neomycin • Halogenated compounds • Parthenium (congress grass) Systemic • NSAIDS • Phenothiazine • Thiazides
Photoallergicreactions Parthenium induced photoallergic dermatitis • A type of hypersensitivity reaction aggravated by sunlight • Commonly seen in people coming in contact with the pollen grains and other parts of the plant Partheniumhysterophorus • Often occurs in farmers and people living in the vicinity of these plants
Polymorphic light eruption (PMLE) • Clinically characterized by an intermittent, delayed, and transient abnormal cutaneous reaction to UVR exposure • The reaction consists of nonscarring, pruritic, erythematous papules, vesicles, or plaques on the light-exposed areas of the skin
Dermatophytid • Eczematous reaction that occurs as an allergic response to a dermatophyte infection elsewhere on the skin Diagnostic criteria • A proven focus of dermatophyte infection. • A positive skin test to a group-specific trichophytin antigen. • Absence of fungi in the dermatophytid lesion. • Clearing of the dermatophytid after the eradication of the primary fungal infection.
Hand eczema • Commonly seen in dermatology practice; can be exogenous, endogenous or of combined aetiology. • Causes discomfort, embarrassment, interferes with normal daily activities. • Common in industrial occupation and threatens job security if infection is not controlled.
Hand eczemaMorphological types • Irritant eczema • Allergic eczema • Recurrent focal palmar peeling • Hyperkeratoticpalmar eczema • Fingertip eczema • Pompholyx (dyshidrotic eczema) • Id reaction
Recurrent focal palmar peeling • A chronic, idiopathic, asymptomatic, non-inflammatory peeling of palms. • Common during summer; often associated with sweaty palms and soles. Occasionally, may involve feet. • Begins with occurrence of round, scaling lesions (2 or 3 mm) on the palms or soles; followed by peeling. • Lesions resolve in 1 to 3 weeks and require no therapy other than lubrication.
Fingertipeczema • Chronic eczema of the palmar surface of the fingertips, which may involve one or all fingertips. • The skin is dry, cracked, scaly and may break down into painful and tender fissures. • Resistant to treatment. • Advise patient to avoid irritants; use topical steroids and maintain lubrication of hands.
Pompholyx (Dyshidroticeczema) • Involves palmar surface of the fingers, palms and soles in which fluid accumulates to form visible vesicles or bullae. • Deep-seated, symmetrical, pruritic, sago grain-like vesicles, preceded by moderate to severe itching. • Vesicles resolve gradually in 3 to 4 weeks, and may be followed by chronic eczematous changes • Cause not known; not associated with any abnormality of the sweat glands.
Hand eczema General instructions to patients • Wash hands infrequently. • Avoid use of soap and wash hands in lukewarm water. • Avoid direct contact with cleansers and detergents. • Avoid direct contact with and/or handling anything that causes burning or itching. E.g. wool; wet nappies; peeling potatoes; handling fresh fruits, vegetables, raw meat. • Preferably wear gloves while doing housework or work that involves contacting irritants. • Ensure frequent use of moisturizers and emollients.
Hand eczema General instructions to patients • Wash hands infrequently. • Avoid use of soap and wash hands in lukewarm water. • Avoid direct contact with cleansers and detergents. • Avoid direct contact with and/or handling anything that causes burning or itching. E.g. wool; wet nappies; peeling potatoes; handling fresh fruits, vegetables, raw meat. • Preferably wear gloves while doing housework or work that involves contacting irritants. • Ensure frequent use of moisturizers and emollients.
Atopicdermatitis • A chronic, immune-mediated, pruritic, inflammatory skin condition. • Marked by alternating periods of remission and flare-ups. • A result of complex interplay between environmental, immunologic, genetic and pharmacologic factors. • Frequently associated with elevated serum IgE levels; personal or family history of atopic dermatitis, allergic rhinitis and/or asthma. • Aggravated by infection, psychological stress, seasonal changes, irritants, and allergens.
AtopicTriad Atopic Dermatitis Allergic Rhinitis Asthma
Atopicdermatitis Diagnosis • It cannot be precisely defined as it does not have specific skin changes, histologic features or diagnostic laboratory test • The diagnosis is usually arrived on the basis of clinical findings, comprising three or more major criteria and three or more minor criteria
Atopicdermatitis Diagnostic criteria: Major features • Pruritus • Typical morphology and distribution • Facial and extensor involvement in infants and children • Flexural lichenification in adults • Chronic or relapsing dermatitis • Personal or family history of atopy (atopic dermatitis; asthma; allergic rhinitis)
Atopicdermatitis Diagnostic criteria: Minor features • Xerosis • Cutaneous infections • Non-specific dermatitis of the hands or feet • Ichthyosis; palmarhyperlinearity; keratosispilaris • Pityriasis alba • Nipple eczema • White dermographism and delayed blanch response • Anterior subcapsular cataracts, keratoconus Contd…
Atopicdermatitis Diagnostic criteria: Minor features • Elevated serum IgE levels • Positive immediate (Type I) skin test reactivity • Early age of onset • Dennie-Morgan infraorbital folds, periorbital darkening • Facial erythema or pallor • Perifollicular accentuation • Course influenced by environmental and/or emotional factors
Atopicdermatitis Clinical features • Age of onset typically during infancy (2 to 6 months); but may start at any age. • Clinical features vary at different phases of life; and comprise: • Itching • Macular erythema, papules or papulo-vesicles • Eczematous areas with crusting • Lichenification and excoriation • Dryness of the skin • Cutaneous reactivity • Secondary infection
Atopicdermatitis Infantile phase (2 months to 2 years) • Sites: cheeks, perioral area and scalp; extensors of feet and elbows • Oozing lesions. • Teething, respiratory infections, emotional upsets and seasonal changes influence the disease course. • The disease often subsides by 18 months of age; but may progress to the childhood phase.
Atopicdermatitis Childhood phase (2 to 12 years) • Characteristically involves elbow and knee flexures, sides of the neck, wrists and ankles. • Scratching and chronicity lead to lichenification. • Hands may often be involved with exudative lesions, sometimes with nail changes. • Secondary bacterial or viral infection may give rise to acute generalized or localized vesiculation.
Atopicdermatitis Adult phase (12 years onwards) • Commonly involves flexural areas. • The disease may be diffuse or patchy. • May manifest only as chronic hand eczema. • Dermatitis of the upper eyelids and blepharitis.
Atopicdermatitis Triggering factors • Anxiety; emotional stress • Temperature change and sweating • Decreased humidity • Excessive washing • Contact with irritants • Allergens • Foods • Microbial agents
Atopicdermatitis Management • First-line treatment • Second-line treatment • Third-line treatment • Counselling; occupational advice
Management of Atopicdermatitis First-line treatment • Identify and control ‘flare factors’ • Topical treatments • Bathing; Emollients; Humectants • Corticosteroids • Calcineurin inhibitors: Pimecrolimus; tacrolimus • Icthamol and tar
Management of Atopicdermatitis First-line treatment • Oral treatment • Antihistamines • Sedative antihistamines preferred • Promethazine; trimeperazine; hydroxyzine • Antibiotics • Systemic steriods (in severe cases)