Download
1 / 19
220 likes | 765 Views
Atopic eczema. Important documents. NICE Clinical Guideline 57, Atopic eczema in children : management of atopic eczema in children from birth up to the age of 12 years, December 2007 Clinical Knowledge Summary (PRODIGY) November 2004 (minor update January 2006). What is atopic eczema?.

E N D
Important documents • NICE Clinical Guideline 57, Atopic eczema in children : management of atopic eczema in children from birth up to the age of 12 years, December 2007 • Clinical Knowledge Summary (PRODIGY) November 2004 (minor update January 2006)
What is atopic eczema? • An itchy inflammatory skin condition with a predilection for the skin flexures. It is characterised by a poorly defined erythema with oedema, vesicles and weeping in the acute stage and skin thickening in the chronic stage
Clinical features and diagnosis • Reduced skin lipid layer > increased transdermal water loss > lowered resistance to irritant substances • Associated with other atopic diseases • Asthma in 30% • Allergic rhinitis in 35% • Children • Prevalence 15-20% • 75% get it by 6m and 80% start < 5 yrs • Clears in 60% by early adolescence • Typically episodic – relapse and remission • Adults • Prevalence 2-10% • Genetic component – present in 80% when both parents affected and 60% when 1 affected
How common is it? • 15-20% of children • 2-10% of adults • Evidence of a 2-3x increase in prevalence over last 30 years • 30% of skin consultations in primary care • 10-20% of dermatology referrals • Unknown cause, multifactorial, recent theory is hygiene hypothesis • Atopic triad • Interaction between genetic susceptibility and environmental triggers
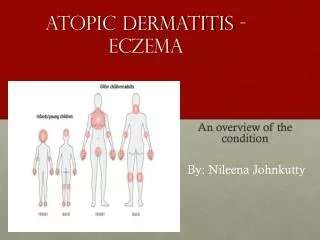
Diagnosis and assessment of children ≤ 12 years • Diagnose atopic eczema when a child up to the age of 12 has an itchy skin condition plus 3 of the following: • Visible flexural dermatitis involving skin creases (elbows, knees) or visible dermatitis on cheeks &/or extensor areas in children ≤18m • Personal history of flexural dermatitis or dermatitis on cheeks &/or extensor areas in children ≤18m • Personal history of dry skin in last 12m • Personal history of asthma or allergic rhinitis (or history of atopy in 1st degree relative of children < 4 years • Onset of signs or symptoms < 2 years
Diagnosis and assessment of children ≤ 12 years • Adopt a holistic approach at each consultation considering : • Severity • Quality of life (everyday activities, sleep, psychosocial wellbeing) • There is not necessarily a direct relationship between severity and its impact on quality of life • Areas of differing severity can coexist in the same child • Treat each area separately
Appearance and distribution • Distribution varies with age, and the appearance of persistent lesions may alter with scratching. The tendency to dry skin persists throughout life • Acute flare ups • Vary in appearance • Poorly demarcated areas, sometimes with crusting, scaling, scratching and swelling of the skin • Chronic lesions • Commonly become thickened (lichenified) as a result of repeated scratching • During infancy • Primarily involves the face, the scalp, the extensor surfaces of the limbs, and is more likely to be acute. Nappy area is usually preserved • In children and adults with long standing disease • Localisation to the flexures of the limbs is more likely • Adults commonly have generalised dryness and itching • Particularly with exposure to irritants
Principles of management in primary care • Identify and avoid provoking factors • Use emollients regularly • Use topical steroids and oral ABs intermittently for flare ups • Refer selected people to specialist • Provide information about : • The condition • Provoking factors • The roles of different Rxs • Effective and safe use of Rxs • Plan treatment considering patient’s goals vs. safety and acceptability of Rx • Demonstrate use of topical treatments emphasising the correct quantities to use
Principles of management in children ≤ 12 years • Identify potential trigger factors • Step up or down depending on severity • Always use emollients even when clear • Potency of corticosteroids should be tailored to severity and body site • Topical tacrolimus and pimecrolimus are not recommended 1st line or for treatment of mild eczema • Offer information on recognition of staph, strep or eczema herpeticum treatment • Spend time educating children and their carers
Managing dry skin • Aim of management of eczema between flare-ups is to : • Control skin dryness and itching • Reduce frequency of flare-ups • Establish a daily skin care regime with emollients • Tailor type, frequency and quantity to patient’s skin requirements and lifestyle • Avoid irritation of the skin • Prescribe a soap substitute • Use gloves when handling irritant substances • Avoid extremes of temperature and humidity • Use non-abrasive clothing fabrics eg cotton • Reapply emollients after wetting the skin
Managing flare-ups • Offer information on : • How to recognise flares • Give instructions on : • How to manage flares according to a stepped care plan • Settle inflammation with topical corticosteroids • Treat clinically apparent bacterial infection with oral ABs • Treatment • Start Rx as soon as signs or symptoms appear • Continue for 48h after symptoms subside • Refer urgently or admit if : • Severe unresponsive disease • Eczema herpeticum is suspected
Managing frequent flare ups • Settle acute flare up • Review and emphasise the use of emollients • Change to one with a higher lipid content • Apply the emollient more often • Apply more emollient each time • Review the factors possibly causing flare ups • Environmental irritants or stresses? • Allergen avoidance is difficult but should be considered if other measures fail • Refer to specialist if : • Risk of adverse systemic effects • Localised adverse effects due to corticosteroid use • Refer to a dietician • In children with 2-3 flares / month • Once controlled use topical corticosteroids on 2 consecutive days / week • Review after 3-6 months to assess effectiveness
Management in adults • Settle chronic lesions • With potent corticosterioid • Review and consider : • Use of emollients • Avoidance of environmental irritants and stress • Antigen avoidance if appropriate • Settle further flare ups • Intermittent use of a topical corticosteroid of appropriate potency and duration of use • Refer to a specialist • Risk of systemic adverse effects • Risk of localised adverse effects from corticosteroid use
Managing severe widespread eczema • Seek specialist help if : • Flare up is widespread, severe, and distressing to the patient • Consider oral prednisolone and antibiotics if : • There is a delay before specialist review • There is a risk of rebound flare up with oral coricosteroids are stopped • Stay on oral corticosteroids until other measures are instituted. Specialist review should occur in 7 days to prevent prolonged drug use
Using oral antihistamines in children • Do not use routinely • Efforts to reduce dryness and inflammation should be promoted ahead of antihistamines • Offer 1 month trial of non-sedating antihistamine to those with severe atopic eczema or those with mild or moderate eczema with severe itching or urticaria • Review Rx every 3 months • Use 7-14 days of a sedating antihistamine if sleep disturbance is significant
When to prescribe an antibiotic • Treat visibly infected eczema with oral antibiotics • Flucloxacillin or erythromycin • Topical antimicrobial / corticosteroid combinations are not more effective than topical corticosteroids alone
When to refer children up to 12 years • Diagnosis is uncertain • Management is not so far satisfactory • Atopic eczema on the face not responding to appropriate Rx • The child or parent may benefit from specialist advice on treatment application (eg bandaging) • Contact allergic dermatitis is suspected • There are significant social or psychological problems • There are severe and recurrent infections
Emollients • Effects • Reduce water loss • Aid softer and suppler skin • May reduce flare ups • Reduce need for steroids • Lack of good quality evidence comparing emollients • Choice depends on patient acceptability • Use the cheapest that is effective and acceptable