Download
1 / 21
210 likes | 384 Views
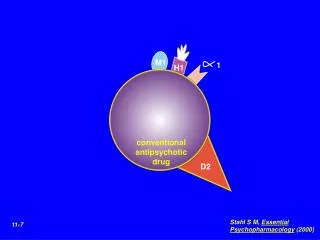
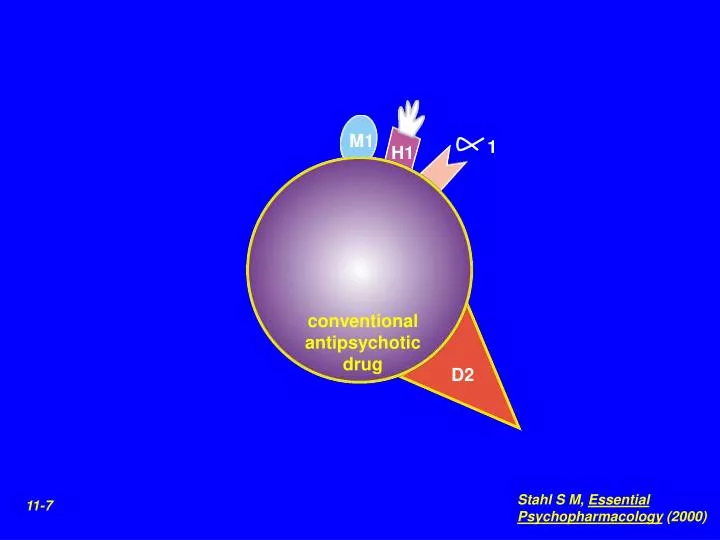
M1. 1. H1. conventional antipsychotic drug. D2. Stahl S M, Essential Psychopharmacology (2000). 11-7. Stahl S M, Essential Psychopharmacology (2000). 11-2. pure D2 blocker. Mesocortical pathway. Increase in negative symptoms. Stahl S M, Essential Psychopharmacology (2000). 11-3.

E N D
M1 1 H1 conventional antipsychotic drug D2 Stahl S M, Essential Psychopharmacology (2000) 11-7
Stahl S M, Essential Psychopharmacology (2000) 11-2 pure D2 blocker
Mesocortical pathway Increase in negative symptoms Stahl S M, Essential Psychopharmacology (2000) 11-3
Nigrostriatal pathway EPSs Stahl S M, Essential Psychopharmacology (2000) 11-4
Blockade of receptors in the nigrostriatal dopamine pathway causes them to up-regulate This up-regulation may lead to tardive dyskinesia Stahl S M, Essential Psychopharmacology (2000) 11-5
Motor and mental features of neuroleptic-induced extrapyramidal side effects Parkinsonism Tremor (resting), rigidity, bradykinesia, masklike facies AkathisiaRestlessness, pacing, fidgeting, shifting from jitteriness, anxiety, irritability, anger, difficulty concentrating DystoniaMuscle contractions, tongue protrusion, torticollis, opisthotonos, fear, distress, paranoia Tardive Buccolingual-masticatory movements of irregular dyskinesia (nonrhythmic) nature; choreiform or athetoid (writhing) movements of fingers, extremities, trunk Adapted from Ayd 1995; Casey 1995
Stahl S M, Essential Psychopharmacology (2000) 11-32 D2 antagonist pituitary lactotroph D2 receptor prolactin
Typical antipsychotic drugs: potencies and side effect profiles Drug Approximate Sedative Hypotensive Anticholinergic Extrapyramidal dose (mg) effect effect effect effect Phenothiazines Chlorpromazine (Thorazine) 100 H H M L Piperidines Thioridazine (Mellaril) 95 H H H L Piperazines Fluphenazine (Prolixin) 2 M L L H Perphenazine (Trilafon) 8 L L L H Trifluoperazine (Stelazine) 5 M L L H Thioxanthene Thiothixene (Navane) 5 L L L H Butyrophenones Haloperidol (Haldol) 2 L L L H
5HT2A SDA D2 Stahl S M, Essential Psychopharmacology (2000) 11-16
brake Substantia nigra brake raphe nucleus Stahl S M, Essential Psychopharmacology (2000) 11-17 5HT-DA Interactions
Stahl S M, Essential Psychopharmacology (2000) 11-18 dopamine neuron dopamine Substantia nigra 5HT2A receptor serotonin 5HT2A receptor serotonin neuron Raphe
Stahl S M, Essential Psychopharmacology (2000) 11-27 mesocortical pathway primary dopamine deficiency dopamine release SDA serotonin secondary dopamine deficiency
Stahl S M, Essential Psychopharmacology (2000) 11-24 Nigrostriatal pathway 5HT2A receptor
5HT1A 1 M1 H1 5HT2A 2 D1 5HT2C D3 5HT3 clozapine 5HT6 D4 D2 5HT7 Stahl S M, Essential Psychopharmacology (2000) 11-37
1 5HT2A 2 risperidone D2 5HT7 Stahl S M, Essential Psychopharmacology (2000) 11-39
1 M1 H1 5HT2A D1 5HT2C D3 5HT3 olanzapine 5HT6 D4 D2 Stahl S M, Essential Psychopharmacology (2000) 11-40
1 H1 5HT2A 2 quetiapine 5HT6 D2 5HT7 Stahl S M, Essential Psychopharmacology (2000) 11-41
5HT1A 1 5HT2A 5HT1D SRI NRI 5HT2C D3 ziprasidone D2 5HT7 Stahl S M, Essential Psychopharmacology (2000) 11-43
Stahl S M, Essential Psychopharmacology (2000) 11-52 polypharmacy combos 3rd line treatment clozapine D2 2nd line treatment D2 noncompliant (depot) SDA 1st line treatment D2 BZ in case of emergency POSITIVE SYMPTOM PHARMACY
Hierarchy of Treatment Goals in Medical Psychotherapy of Schizophrenia • Acute Phase • Medical/neuropsychiatric assessment • Rapid symptom reduction • Reduce impact of episode on friends, family, housing, activities • Convalescent Phase • Gain trust/alliance with family/caregivers • Assess and mobilize social supports • Ensure human service needs are met (food, clothing, housing) • Ensure safety and predictability of environment • Adaptive Plateau • Establish therapeutic alliance/supportive treatment routine • Achieve effective maintenance medication regime • Stable plateau • Psychoeducation: Promote illness self-management strategies, awareness of relationship between stress and symptoms • Rehabilitation: Teach adaptive competencies