Download
1 / 45
550 likes | 1.31k Views
Pharmacology of Antipsychotic drug s. Antipsychotic drugs, neuroleptic or anti-schizophrenic drugs are used mainly to manage psychosis (including delusions or hallucinations and disordered thought ) particularly in schizophrenia and bipolar depression. Schizophrenia.

E N D
Antipsychotic drugs, neuroleptic or anti-schizophrenic drugs are used mainly to manage psychosis (including delusions or hallucinations and disordered thought ) particularly in schizophrenia and bipolar depression
It is a chronic disabling disorder which affects people during late adolescence or early adulthood Schizophrenia has a strong genetic component and is probably due to biochemical abnormality (dysfunction of D-ergic neurons) There is some evidence for involvement of 5-HT
Patients with schizophrenia have problems with seeing things, hearing voices, imagining things, having terrifying thoughts (positive symptoms) Apathy , blunted emotions, anhedonia and reduced ability to react with people ‘social withdrawal’ (Negative symptoms)
Schizophrenia: Symptoms • Negative Symptoms • Blunted emotions • Social withdrawal • Loss of motivation • impaired personal hygiene • Positive Symptoms • Hallucinations • Delusions • Thought disturbances
“Dopamine hypothesis” Schizophrenia has a strong genetic component and probably reflects too much dopamine activity in themesolimbic systemwhich isthe part of brain that controls seeing, hearing, imaging etc…..
“Dopamine hypothesis” - Evidences • Drugs that increase dopamine may produce positive psychotic symptoms (e.g. Cocaine, amphetamine) • All known antipsychotics drugs capable of treating positive psychotic symptoms block the dopamine receptors (D2)
Antipsychotics are broadly divided into two groups: The typical = 1st generation and the atypical = 2nd generation antipsychotics Atypical drugs are preferred as a first line treatment because they: 1- have fewer side effects 2- have additional benefits for the “ -ve symptoms”of schizophrenia
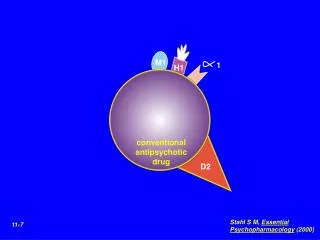
All antipsychotic drugs block D2 receptors in the brain & periphery Atypical antipsychotics exert part of their action through blocking of 5-HT2A receptors Antipsychotics take days or weeks to work, suggesting that secondary effects (e.g. increase in number of D2-receptors in limbic structure) may be more important than direct effect of D2-receptor block.
Many antipsychotics block other receptors e.g. acetylcholine (M), noradrenaline (α ) and histamine (H1) receptors
Typical antipsychotic Drugs 1- Phenothiazine derivatives: Chlorpromazine, promethazine, Fluphenazine 2- Butyrophenone derivatives: Haloperidol, droperidol Atypical antipsychotic drugs Risperidone , Clozapine , Olanzapine Aripiprazole
1- Antipsychotic effects Though blocking D2 receptors in the mesolimbic system, antipsychotic drugs relieve hallucination, improve thoughts. The additional blocking effects of atypical antipsychotics on 5-HT2 receptors can treat the negative symptoms of schizophrenia 2- Autonomic effects: Anticholinergic effects , dry mouth, constipation and blurred vision Blocking of α–adrenergic receptors hypotension
3- Exrapyramidal effects Blocking of D2 receptors in the nigrostriatal pathway causes unwanted parkinsonian-like symptoms; rigidity and tremors. Clozapine and risperidone exhibit a low incidence of these symptoms ( block D4) 4- Antiemetic effect Blocking D2 receptors both centrally in the CTZ in the medulla and peripherally in the stomach
5- Endocrine effects: Amenorrhea-galactorrhea, false–positive pregnancy tests in women and decreased libido and gynecomastia in men (due to blockade of D2 in the pituitary leading to an increase in prolactin release) 6-Antipsychotics block H1 receptors causing sedation and confusion 7-Antipsychotic depress the hypothalamus affecting thermo-regulation (hypothermia)
1- Treatment of schizophrenia • Typical antipsychotics are most effective in treating positive symptoms • Atypical antipsychotics with serotonin blocking activity are effective in many patients resistant to the traditional agents, especially in treating negative symptoms
2- Treatment of other psychotic disorders e.g. mania and mood (bipolar) disorders 3- Prevention of severe nausea and vomiting (drug-induced nausea) 4-Droperidolis used in combination with fentanyl in neuroleptanalgesia
5-Due to its antihistaminic effects, promethazine is used in cases of pruritus and as a preoperative sedative 6- To induce hypothermiain certain major operations (Chlorpromazine) 7- Chlorpromazine is used to treat intractable hicough حازوقه
Extrapyramidal Symptoms (EPS)Dopamine Vs Acetylcholine • Dopamine (inhibitory) and ACh (excitatory) have a reciprocal relationship in the Nigrostriatal pathway • A delicate balance allows for normal movement • Dopamine blockade by antipsychotic drugs results in relative increase in cholinergic activity causing EPS • When high potency antipsychotics are chosen, we often prescribe anticholinergic medication like benztropine
Antipsychotics have a wide range of side effects 1- Sedation (drowsiness) is a common side effect of antipsychotics (?) This can be dealt with by taking medication at night just before going to bed 2- Movement disorders;Extrapyramidal side effects are common with the typical antipsychotics ; include dystonia, akathisia parkinsonian- like syndromeTreatment: anticholinergic drugs (benztropine)
Tardive dyskinesia • It is the most important adverse effect of long-treatment with typical antipsychotic drugsand is characterized by excessive movement of the lips, tongue and jaw, limbs • Tardive dyskinesia may be irreversible and is postulated to result from increased number of dopamine receptors that are synthesized in response to long-term dopamine receptor blockade, which leads to neuronal supersensitivity to dopamine
Atypical drugs have lower incidence of EPS & tardive dyskinesia as they block 5-HT2A receptors and have less D2 receptor blocking effect
3-Autonomic effects:Orthostatic hypotension !!!!, (α-adrenoceptor blockade) and anticholinergic adverse effects (urinary retention,constipation, ppt of glaucoma,…..) 4- Endocrine and metabolic effects: hyperprolactinemia in the form of galactorrhea, amenorrhea in women, gynecomastia and changes in libido & impotence in men
5- Allergic reactions: Agranulocytosis (common with clozapine), cholestatic jaundice and skin eruptions 6-Occular complications: may cause retinal pigmentation, corneal and lens opacities (Chlorpromazine) 7- Clozapine and chlorpromazine tend tolower an individual’s seizure threshold
Neuroleptic Malignant Syndrome • An idiosyncratic,life-threatening neurological disorder associated with antipsychotic therapy • Idiosyncracy: An unusual or unexpected sensitivity exhibited by an individual to a particular food or drug. Idiosyncrasy is usually determined genetically and it may be due to a biological deficiency (e.g. an inability to metabolize a drug).
Neuroleptic Malignant Syndrome • Clinical manifestations include: • Encephalopathy, Hyperpyrexia, delirium • Autonomic instability (BP) • Rigidity of muscles • Elevated creatinephosphokinse(CPK)due to increased muscular activity and rhabdomyolysis(destruction of muscle tissue)
Pathophysiology The mechanism is thought to depend on dopamine activity due to: • Dopamine receptor blockade • Genetically reduced function of dopamine receptor • There is an increased calcium release from the sarcoplasmic reticulum of muscle cells which can result in rigidity and cell breakdown
Treatment involves: • Immediate discontinuation of antipsychotic drug • Treat hyperthermia • Hydration, maintain vital functions • Dantrolene sodium: a muscle relaxant that acts by abolishing excitation contraction coupling in muscle cell
Chlorpromazine • Phenothiazine class • Increased prolactin (gynaecomastia) • Hypothermia • Anticholinergic effects • Hypersensitivity reactions • Obstructive jaundice • Ocular complications • EPS
Fluphenazine • Phenothiazine class but: • does not cause jaundice • causes less hypotension • causes more EPS
Halopirodol • Butyrophenone class • As chlorpromazine but does not cause jaundice • Fewer anticholinergic side effects • Strong EPS tendency
Differences between typical and atypical groups • receptor profile • Serotonin receptors (5-HT2A) are involved • incidence of extrapyramidal side effects (less in atypical group) • efficacy (specifically of Clozapine in treatment of resistant group of patients • efficacy against negative symptoms
Clozapine • Dibenzodiazepine class • Potent antagonist at D4-receptors • Selectively blocks 5-HT2A receptors • Sedation • Extrapyramidal side effects are minimal • Low incidence of Tardive dyskinesia • Increased risk for seizures (2-3%)
Clozapine • Agranulocytosis in 1% (regular granulocyte counts weekly is required) • Agranulocytosis risks increase when co-administered with carbamazepine • Anticholinergic side effects • Weigh gain • Shows efficacy in 'treatment-resistant' patients • Effective against negative and positive symptoms
Risperidone • Largely replacing clozapine. No risk of agranulocytosis • Low incidence of EPS and minimal sedation • Weight gain • Resperidone is approved for the treatment of autism and bipolar depression
Aripiprazole • Recently approved drug • Long acting (plasma half-life ∼3 days) • No effect on prolactin secretion • No weight gain • Less incidence of dystonias and Tardive dyskinesia • D2 partial agonist profile may account for paucity of side effects
Advantages & disadvantages of Clozapine Advantages Disadvantages Clozapine has the risk of inducing agranulocytosis Clozapine tends to lower an individual seizure threshold • Effective in the treatment of negative and positive symptoms of schizophrenia • More effective than classical agents for resistant cases
Advantages Disadvantages Atypical drugs cause weigh gain Atypical drugs may exacerbate DM & hyperlipidemia Are more expensive than typical antipsychotics • Incidence of extrapyramidal symptoms is lowest • Tardive dyskinesia is extremely rare with clozapine