Download
1 / 14
150 likes | 236 Views
Learn about psoriatic arthritis, including its symptoms, diagnosis criteria, subtypes, extra-articular findings, and treatment options. Discover how to diagnose patients without skin manifestations and understand the course and prognosis of this inflammatory condition.

E N D
Psoriatic Arthritis • Emily Chang • Morning Report • August 14, 2009 • August
Definition • Inflammatory arthritis associated with psoriasis • Usually seronegative for Rheumatoid Factor • Classified with HLA-B27-associated spondyloarthropathies
Epidemiology • Likely in up to 25-34% of patients with presence of skin disease • Overall prevalence 0.04-1.2% • M=F although it differs in subsets • Peak age of onset between 30-55 years
CASPAR criteria • evidence of psoriasis • current - 2 • history of - 1 • family history of - 1 • psoriatic nail dystrophy (onycholysis, pitting, hyperkeratosis) • negative rheumatoid factor • dactylitis, either current or history of • radiological evidence of juxta-articular new bone formation
Subtypes • DIP joint pattern • oligoarticular (<5 joints) pattern, usually assymetric • polyarticular (>=5 joints), symmetric in half • arthritis mutilans • spondyloarthritis
Other Rheum Findings • enthesitis (inflammation at site of tendon insertion) • tenosynovitis (inflammation of tendon and its enveloping sheath) • dactylitis or “sausage digit”
Extra-articular findings • skin - psoriasis • nails - pits and onycholysis • pitting edema - often asymmetrical • ocular inflammation - conjunctivitis, iritis
How to diagnose those without skin findings • look for distal joint involvement in asymmetric distribution • look at the nails • look in ears • ask about family history • dactylitis
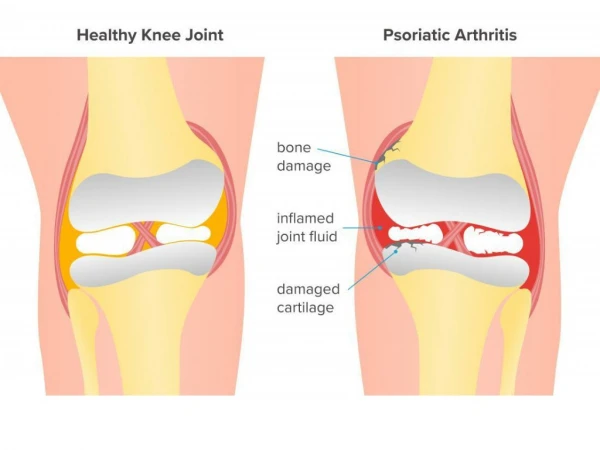
Diagnostic Testing • no diagnostic laboratory testing • radiologically: • erosive changes and new bone formation in distal joints • lysis of terminal phalanges • fluffy periostitis and new bone formation at sites of enthesitis • “pencil in cup” appearance
Differential • Reactive (Reiter’s) Arthritis • Rheumatoid Arthritis with concomitant psoriasis • ankylosing spondylitis • gouty arthritis
Treatment • NSAIDs if disease is mild. • PT, OT, splinting devices • If erosive disease, treat aggressively with DMARDs (MTX, Sulfasalazine, CsA). • If skin disease is the major issue, should be managed by a dermatologist. • Early referral to rheumatology for initiation of DMARDs to prevent progression.
Course and Prognosis • 20% of patients have a severe an debilitating form of arthritis • originally thought to be more benign course than RhA • progression of clinical damage occurs in a majority of patients • radiologic changes occur over time despite treatment
References • Klippel, John. Primer on the Rheumatic Diseases. Edition 12. Atlanta, GA: Arthritis Foundation; 2001: 584-586. • Gladman, Dafna. Psoriatic arthritis. Dermatologic Therapy. Vol 22. 2009, 40-55. • www.utdol.com