Download
1 / 18
321 likes | 2.04k Views
Psoriatic Arthritis. Shahrad Behnam MS IV. INTRODUCTION. Psoriasis is a hyper-inflammatory disease that contributes to the development of demarcated erythematous scaly plaques.

E N D
Psoriatic Arthritis Shahrad Behnam MS IV
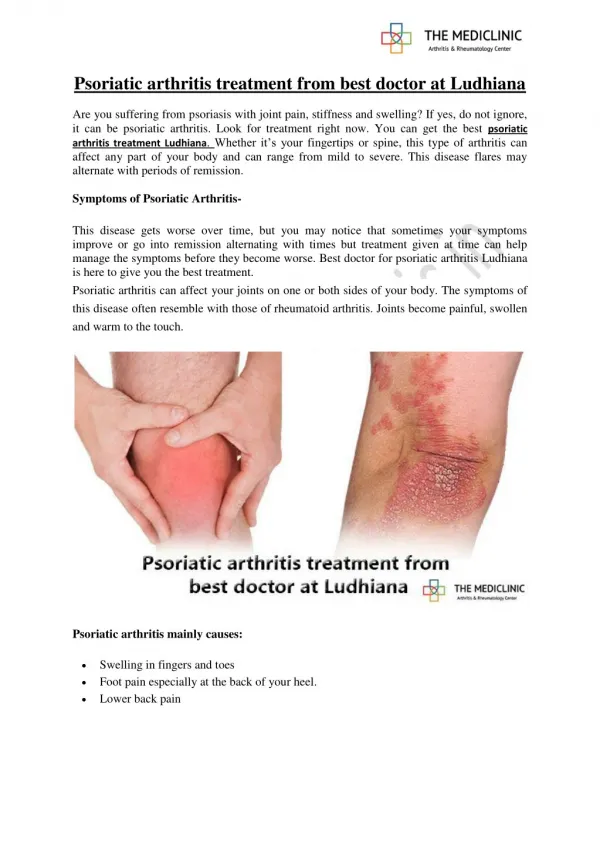
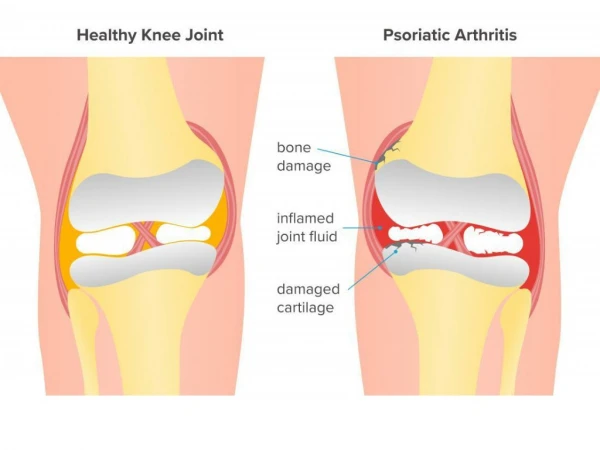
INTRODUCTION • Psoriasis is a hyper-inflammatory disease that • contributes to the development of demarcated • erythematous scaly plaques. • Psoriatic arthritis is due to inflammation in and around the joints, usually the wrists, knees, ankles, lower back and neck. • Up to 30% of psoriasis patients may develop psoriatic arthritis. • On average, psoriatic arthritis appears about 10 years after first signs of psoriasis. • 60-80% of patients with psoriatic arthritis may have psoriasis. • Majority have a negative Rheumatoid Factor, and it is usually referred to as "seronegative arthritis.” psoriasis of knees
DIAGNOSIS • Diagnosis of psoriatic arthritis depends on both clinical and radiological assessments. • The presence of an inflammatory arthritis in a patient with psoriasis makes the diagnosis likely.
CLINICAL PRESENTATION • Pattern of joints affected with psoriatic arthritis is different than those with rheumatoid arthritis. Rheumatoid arthritis Psoriatic arthritis The high frequency of distal joint involvement in psoriatic arthritis compared to rheumatoid arthritis.
CLINICAL PRESENTATION • Symptoms/Sings: • Morning stiffness lasting more than 30 minutes. • Patients present with pain and stiffness and swelling in the affected joints. • Nail changes are found in 80-90% of patients with psoriatic arthritis and include the following: • Onycholysis (elevation of the nail bed), and nail pitting (see below).
RADIOLOGICAL DEFORMITIES • There is coexistence of erosive changes and new bone formation in distal joints. • “cup-and-pencil deformity” is erosion of one end of bone with expansion of the base of the contiguous bone. • Resorption of tufts of terminal phalanges. • There is usually no osteoporosis. Osteoporosisoccurs in RA. • Joint-space widening or narrowing. • Periosteal bone formation. • There may be surrounding soft tissue swelling (dactilitis). • Presence of anykolysis: intra-articular bone fusion, specially of DIP and PIP joints.
RADIOLOGICAL DEFORMITIES • Sacroiliitis: inflammation of the sacro-illiac joints, which lead to erosions and sclerosis of SI joints. • Spondylitis: Inflammation of one or more vertebrae, which may lead to paravertebral ossification. • Enthesitis: Inflammation at the site of tendon insertion into bone, ie of the achilles tendon. • Arthritis mutilans: Destructive changes and joint deformity of the hand and pan-compartmental ankylosis of the wrist.
5 Patterns of Psoriatic Arthritis • 1. Symmetrical polyarthritis • Most common type, may affect as much as 25% of patients. • The hands, wrists, ankles, and feet may be involved. • It can be differentiated from RA by • Characteristic radiographic findings (as noted above) • A history of psoriasis • Presence of DIP involvement • Absence of subcutaneous nodules on xray • A negative rheumatoid factor
5 Patterns of Psoriatic Arthritis • 2. Asymmetrical oligoarticular arthritis • 2nd most common form of presentation. • As many as 4 large joints may be affected, often with acute scattered involvement of the metatarsophalangeal, PIP and DIP joints. • Dactylitis (sausage digits) may be present.
5 Patterns of Psoriatic Arthritis • 3. Distal interphalangeal (DIP) arthropathy • DIP joint involvement occurs in 5-10% of patients with psoriatic arthritis. • One or several DIP joints may be involved. • Clinically, there is periarticular swelling and acute inflammation with warmth. UpToDate.com UpToDate.com
Radiograph of both hands demonstrates cup-in-pencil deformities of both thumbs and erosion of DIP joint of left middle finger
#3 #2 #1 A more closer look of pencil-in-cup deformity (#1) , along with articular ankylosis (#2) at the site of DIP and osteolysis of distal phalangeal (#3)
5 Patterns of Psoriatic Arthritis • 4. Arthritis mutilans • Occurs in 5% of patients with psoriatic arthritis. UpToDate.com UpToDate.com
5 Patterns of Psoriatic Arthritis • 5. Spondyloarthropathy • This includes both sacroiliitis and spondylitis. • Clinical evidence of spondylitis, sacroiliitis, or both can occur in conjunction with • other subgroups of psoriatic arthritis. Bilateral sacroiliitis is most common. There are erosion and sclerosis at the SI joints (arrows)
Normal spine: In un-diseased spine, there is concavity of vertebral bodies (arrows).
#2 #1 • Spondylitis may occur without radiologic evidence of sacroiliitis and may appear radiologically without the classic symptoms of morning stiffness in the lower back. • With spondylitis, there is loss of the concavity of the vertebral body, resulting in squaring of the vertebral bodies (arrow #1). There is also fusion of vertebral bodies (arrow #2) due to bridging syndesmophytes resulting in bamboo spine.
MANAGEMENT OPTIONS: • Nonsteroidal Anti-inflammatory Drugs (NSAIDs) • COX-2 inhibitors • Both NSAIDS and Cox-2 inhibitors are used to control the inflammation and help improve patient’s quality of life. But they do not stop the progression of underlying disease (erosion) and may not be efficacious long term. Cox-2 inhibitors are being used less due to cardiovascular side effects. • Disease Modifying Antirheumatic Drugs (DMARDS) • (ie) Methotrexate, Cyclosporine or Azathioprine • These agents slow or stop the progression of disease and joint erosion. However, their side effects profile (liver and kidney damage, immune suppression, cancers) prevent long term use. • Biologics: • Agents that are synthesized by recombinant DNA technology and target specific proteins or cytokines. These agents are gaining momentum rapidly. They stop progression of disease and are so far well tolerated. • Enbrel (etanercept) is the only biologic so far approved for psoriatic arthritis. Unfortunately, it is extremely expensive (Enbrel costs $15,000/yr).
References: [1] Zachariae, H. Prevalence of joint disease in patients with psoriasis: implications for therapy. Am J Clin Dermatol 2003; 4:441 [2] Brockbank, J, Gladman, D. Diagnosis and management of psoriatic arthritis. Drugs 2002; 62:2447. [3] Dafna D Gladman, Clinical manifestations and diagnosis of psoriatic arthritis, UpToDate.com [4] Dafna D Gladman, Treatment of psoriatic arthritis. [5] Finucane KA, Archer CB. Recent advances in rheumatology: biological agents for the treatment of rheumatoid arthritis, the progression of psoriatic arthritis, autoantibodies in systemic lupus erythematosus. Clin Exp Dermatol. 2005 Mar;30(2):201-4.