Download
1 / 1
10 likes | 131 Views
PREDICTORS OF DIABETIC WOUND HEALING BY RACIAL/ETHNIC CATEGORIES . Ranjita Misra 1 , Lynn Lambert 2 , David Vera 3 , Ashley Mangaraj 3 , Suchin R Khanna 3, Chandan K Sen 3.

E N D
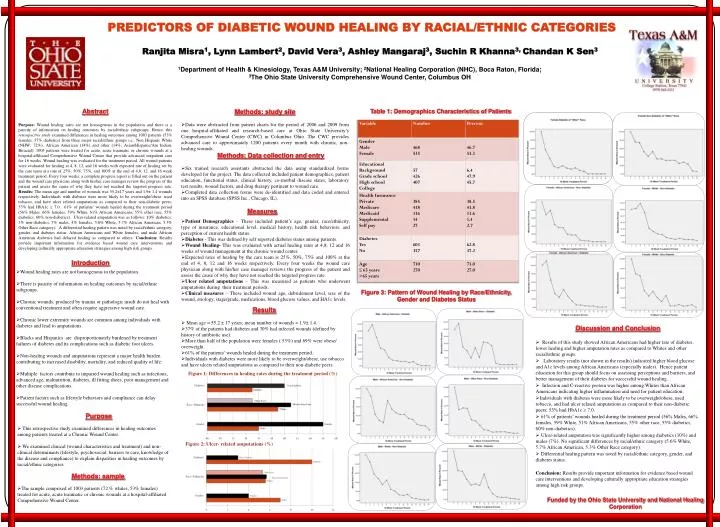
PREDICTORS OF DIABETIC WOUND HEALING BY RACIAL/ETHNIC CATEGORIES RanjitaMisra1, Lynn Lambert2, David Vera3, Ashley Mangaraj3, Suchin R Khanna3, Chandan K Sen3 1Department of Health & Kinesiology, Texas A&M University; 2National Healing Corporation (NHC), Boca Raton, Florida; 3The Ohio State University Comprehensive Wound Center, Columbus OH Abstract Purpose: Wound healing rates are not homogenous in the population and there is a paucity of information on healing outcomes by racial/ethnic subgroups. Hence, this retrospective study examined differences in healing outcomes among 1003 patients (53% females, 37% diabetics) from three major racial/ethnic groups i.e., Non Hispanic White (NHW; 72%), African American (14%) and other (14%; Asian/Hispanic/Am Indian, Biracial). 1003 patients were treated for acute, acute traumatic or chronic wounds at a hospital-affiliated Comprehensive Wound Center that provide advanced outpatient care for 16 weeks. Wound healing was evaluated for the treatment period. All wound patients were evaluated for healing at 4, 8, 12, and 16 weeks with expected rate of healing set by the care team at a rate of 25%, 50%, 75%, and 100% at the end of 4,8, 12, and 16 week treatment period. Every four weeks, a complete progress report is filled out on the patient and the wound care physician along with his/her case manager review the progress of the patient and assess the cause of why they have not reached the targeted progress rate. Results: The mean age and number of wounds was 55.2±17 years and 1.9± 1.4 wounds respectively. Individuals with diabetes were more likely to be overweight/obese, used tobacco, and have ulcer related amputations as compared to their non-diabetic peers; 53% had HbA1c ≥ 7.0. 61% of patients’ wounds healed during the treatment period (56% Males, 66% females, 59% White, 61% African Americans, 55% other race, 55% diabetics, 60% non-diabetics). Ulcer-related amputation was as follows: 10% diabetics, 3% non-diabetics, 7% males, 4% females, 5.6% White, 5.7% African American, 5.3% Other Race category). A differential healing pattern was noted by racial/ethnic category, gender, and diabetes status. African Americans and White females, and male African American diabetics had delayed healing as compared to others. Conclusion: Results provide important information for evidence based wound care interventions and developing culturally appropriate education strategies among high risk groups. • Methods: study site • Data were abstracted from patient charts for the period of 2006 and 2009 from one hospital-affiliated and research-based care at Ohio State University’s Comprehensive Wound Center (CWC) in Columbus Ohio. The CWC provides advanced care to approximately 1200 patients every month with chronic, non-healing wounds. • Methods: Data collection and entry • Six trained research assistants abstracted the data using standardized forms developed for the project. The data collected included patient demographics, patient education, functional status, clinical history, co-morbid disease states, laboratory test results, wound factors, and drug therapy pertinent to wound care. • Completed data collection forms were de-identified and data coded and entered into an SPSS database (SPSS Inc., Chicago, IL). • Measures Table 1: Demographics Characteristics of Patients • Patient Demographics – These included patient’s age, gender, race/ethnicity, type of insurance, educational level, medical history, health risk behaviors, and perception of current health status. • Diabetes - This was defined by self reported diabetes status among patients. • Wound Healing- This was evaluated with actual healing rates at 4,8, 12 and 16 weeks of wound management at the chronic wound center. • Expected rates of healing by the care team is 25%, 50%, 75% and 100% at the end of 4, 8, 12 and 16 weeks respectively. Every four weeks the wound care physician along with his/her case manager reviews the progress of the patient and assess the cause of why they have not reached the targeted progress rate. • Ulcer related amputations – This was measured as patients who underwent amputations during their treatment periods. • Clinical measures – These included wound age, debridement level, size of the wound, etiology, stage/grade, medications, blood glucose values, and HA1c levels. • Wound healing rates are not homogenous in the population. • There is paucity of information on healing outcomes by racial/ethnic subgroups. • Chronic wounds, produced by trauma or pathologic insult do not heal with conventional treatment and often require aggressive wound care. • Chronic lower extremity wounds are common among individuals with diabetes and lead to amputations. • Blacks and Hispanics are disproportionately burdened by treatment failures of diabetes and its complications such as diabetic foot ulcers. • Non-healing wounds and amputations represent a major health burden contributing to increased disability, mortality, and reduced quality of life. • Multiple factors contribute to impaired wound healing such as infections, advanced age, malnutrition, diabetes, ill fitting shoes, poor management and other disease complications. • Patient factors such as lifestyle behaviors and compliance can delay successful wound healing. Introduction Figure 3: Pattern of Wound Healing by Race/Ethnicity, Gender and Diabetes Status • Results • Mean age = 55.2 ± 17 years; mean number of wounds = 1.9± 1.4. • 37% of the patients had diabetes and 30% had infected wounds (defined by history of antibiotic use). • More than half of the population were females ( 53%) and 69% were obese/ overweight. • 61% of the patients’ wounds healed during the treatment period. • Individuals with diabetes were more likely to be overweight/obese, use tobacco and have ulcers related amputations as compared to their non-diabetic peers. • Discussion and Conclusion • Results of this study showed African Americans had higher rate of diabetes, lower healing and higher amputation rates as compared to Whites and other racial/ethnic groups. • Laboratory results (not shown in the results) indicated higher blood glucose and A1c levels among African Americans (especially males). Hence patient education for this group should focus on assessing perceptions and barriers, and better management of their diabetes for successful wound healing. • Infection and C-reactive protein was higher among Whites than African Americans indicating higher inflammation and need for patient education. • Individuals with diabetes were more likely to be overweight/obese, used tobacco, and had ulcer related amputations as compared to their non-diabetic peers; 53% had HbA1c ≥ 7.0. • 61% of patients’ wounds healed during the treatment period (56% Males, 66% females, 59% White, 51% African Americans, 55% other race, 55% diabetics, 60% non-diabetics). • Ulcer-related amputation was significantly higher among diabetics (10%) and males (7%). No significant differences by racial/ethnic category (5.6% White, 5.7% African American, 5.3% Other Race category). • Differential healing pattern was noted by racial/ethnic category, gender, and diabetes status. • Conclusion: Results provide important information for evidence based wound care interventions and developing culturally appropriate education strategies among high risk groups. Figure 1: Differences in healing rates during the treatment period (%) • This retrospective study examined differences in healing outcomes among patients treated at a Chronic Wound Center. • We examined clinical (wound characteristics and treatment) and non-clinical determinants (lifestyle, psychosocial, barriers to care, knowledge of the disease and compliance) to explain disparities in healing outcomes by racial/ethnic categories. • The sample comprised of 1003 patients (72 % whites, 53% females) treated for acute, acute traumatic or chronic wounds at a hospital-affiliated Comprehensive Wound Center. Purpose Figure 2: Ulcer- related amputations (%) Methods: sample Funded by the Ohio State University and National Healing Corporation