Download
1 / 16
160 likes | 319 Views
UOG Journal Club: July 2011. Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix: a multicenter, randomized, double-blind, placebo-controlled trial S. S. Hassan, R. Romero, D. Vidyadhari et al . for the PREGNANT Trial

E N D
UOG Journal Club: July 2011 Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix: a multicenter, randomized, double-blind, placebo-controlled trial S. S. Hassan, R. Romero, D. Vidyadhari et al. for the PREGNANT Trial Volume 38, Issue 1, Date: July 2011, pages 18–31 Journal Club slides prepared by Dr Asma Khalil (UOG Editor for Trainees)
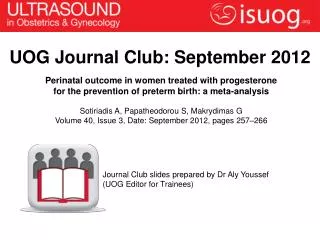
60 50 40 Perinatal mortality (%) 30 20 10 0 24 25 26 27 28 29 30 31 32 33 34 Gestation (weeks) Preterm birth Leading cause of perinatal morbidity and mortality Centre for Maternal and Child Enquiries (CMACE) Perinatal Mortality 2009:UK Mathews TJ et al., Natl Vital Stat Rep 2000
Detection rate (FPR 10%) Cervical length+ Obstetric Hx + Maternal characteristics Obstetric Hx + Maternal characteristics Cervical length Cervical length+ Obstetric Hx Preterm birth PTB < 28 weeks 76 81 82 23 PTB 28 – 30 weeks 57 59 62 35 PTB 31 – 33 weeks 47 53 55 32 PTB 34 – 36 weeks 24 29 29 23 Cervical length is the best predictor for preterm birth • For every 100,000 women screened, $12 million can be saved and 22 cases of neonatal death or long-term neurologic deficits prevented • Universal cervical length screening is cost-effective Celik E et al., UOG 2008 Werner EF et al., UOG 2010
Proposed strategies to reduce the risk of preterm birth Pessary Progesterone Cerclage Preterm birth prevention Mechanism of action of progesterone • Not well understood • Exerts biological effects on the chorioamniotic membranes and cervix (Yellon S et al., ReprodSci 2009) • Prevents cervical ripening (Xu H et al., AJOG 2008) • Suppresses uterine smooth muscle activity (Grazzini E et al., Nature 1998)
Progesterone versus placebo Prevention of PTB RCTs included Total RR 95% CI Past Hx of spontaneous PTB* da Fonseca 2003 0.15 0.04 – 0.64 142 Sonographic short cervix* Fonseca 2007 250 0.58 0.38 – 0.87 Multiple pregnancy#† NS NS 732 Hartikainen 1980; Rouse 2007 Prior threatened PTB#† Facchinetti 2007 60 0.29 0.12 – 0.69 Prenatal administration of progesterone for prevention of preterm birth (Cochrane Review) *Preterm birth < 34 weeks #Preterm birth < 37 weeks †17-alpha hydroxyprogesterone caproate Dodd JM et al., Cochrane Review 2009
Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix Hassan et al., UOG 2011 Phase III, prospective, randomized, placebo-controlled, double-masked, parallel-group, multi-center, international trial. Objective To determine the efficacy and safety of vaginal progesterone gel in reducing the rate of PTB < 33 weeks in asymptomatic women with a mid-trimester sonographic short cervix.
Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix Hassan et al., UOG 2011 Methodology • Inclusion criteria • Singleton • GA 19+0 – 23+6 weeks • Cervical length (TV US): 10 – 20 mm • Asymptomatic (no symptoms or signs of preterm labor) • Exclusion criteria • Planned cerclage • Acute cervical dilation • Allergy to progesterone • Recent progestogen treatment (within 4 weeks) • Chronic medical conditions • Major fetal anomaly or chromosomal abnormality • Uterine malformations • Vaginal bleeding • Known/suspected chorioamnionitis
Outcomes • Secondary outcomes • Neonatal morbidity • RDS • Bronchopulmonary dysplasia • Intraventricular hemorrhage (Grade III or IV) • Periventricular leukomalacia • Sepsis • Necrotizing enterocolitis • Perinatal mortality • PTB <28, <35, and <37 weeks • Neonatal biometry at birth • Congenital abnormalities Primary outcome Preterm birth <33 weeks
Analysis sets Compliant analysis Treated patient analysis Intent-to-treat analysis All patients randomized to either vaginal progesterone or placebo Patients who took at least one dose of either placebo or progesterone Patients who used at least 80% of study medication, no cerclage and no loss to follow-up Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix Hassan et al., UOG 2011
ITT analysisTreated patientCompliant analysis Adjusted* Adjusted* Unadjusted P value P value P value Outcome Preterm birth PTB < 28 weeks 0.04 NS 0.04 PTB < 33 weeks† 0.02 0.02 0.01 PTB < 35 weeks 0.02 0.01 0.01 PTB < 37 weeks NS NS NS Neonatal morbidity RDS 0.03 0.04 NS 0.04 NS NS Any morbidity/mortality Birth weight < 1500g 0.01 0.01 0.01 †Primary study outcome *Adjustment for study site and risk strata
Progesterone for the prevention of preterm birth in women with short cervix 25 50 20 40 30 15 Preterm birth < 34 weeks (%) Preterm birth < 33 weeks (%) 44% 45% 20 10 34% 16% 19% 9% 10 5 0 0 Placebo N=235 Progesterone N=223 Placebo N=125 Progesterone N=125 N = 250 Cervix: 15 mm (median 11.5 mm) GA: 20 – 25 weeks (median 22 weeks) Progesterone capsule 200 mg PV daily Duration: 20 – 34 weeks No serious adverse events Fonseca EB et al., NEJM 2007 N = 458 Cervix: 10 to 20 mm (median 18 mm) GA: 20 – 23+6 weeks (median 22 weeks) Progesterone bioadhesive gel 90 mg PV daily Duration: 20 – 36+6 weeks No serious adverse events Hassan S et al., UOG 2011
Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix Hassan et al., UOG 2011 Treatment-related adverse events • There was no difference in the incidence of treatment-related adverse events between the groups (p=0.51): • Vaginal pruritus • Vaginal discharge • Vaginal candidiasis • Nausea No fetal or neonatal safety signal was detected for vaginal progesterone gel One case of congenital anomaly in the progesterone group and three in the placebo group
NNT Progesterone for prevention of PTB < 33 weeks* 14 Progesterone for prevention of RDS* 22 Clinical utility – Number needed to treat (NNT) to prevent adverse outcome MgSO4 for prevention of eclampsia† 100 Antenatal steroids for prevention of RDS‡ 13 Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix Hassan et al., UOG 2011 *Hassan S et al., UOG 2011 †Altman D et al., Lancet 2002 ‡Sinclair JC et al., AJOG1995
Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix Hassan et al., UOG 2011 Strengths • Multicenter • Placebo-controlled • Double-blind RCT • Rigorous standards for the allocation and concealment of treatment • Additional sensitivity analysis in the ITT analysis set to provide a “worst case” scenario • Primary results are consistent with the literature • Preterm delivery rate in the placebo arm is similar to that reported in other studies • Multi-national nature of the trial The first study to show improvement in neonatal morbidity
Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix Hassan et al., UOG 2011 Limitations In the “compliant analysis set”, there was no improvement in the neonatal morbidity apart from increased birth weight • The primary endpoint is a surrogate for infant outcome • Not powered to detect differences in outcome according to risk strata (presence or absence of a previous preterm birth)
Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix Hassan et al., UOG 2011 Conclusion Vaginal progesterone reduces the rate of preterm birth before 33 weeks of gestation and improves neonatal outcomes in women with a sonographic short cervix • Discussion • Should we undertake universal mid-trimester cervical length screening? • Should vaginal progesterone gel be administered to women with a short cervix?