Download
1 / 27
280 likes | 432 Views
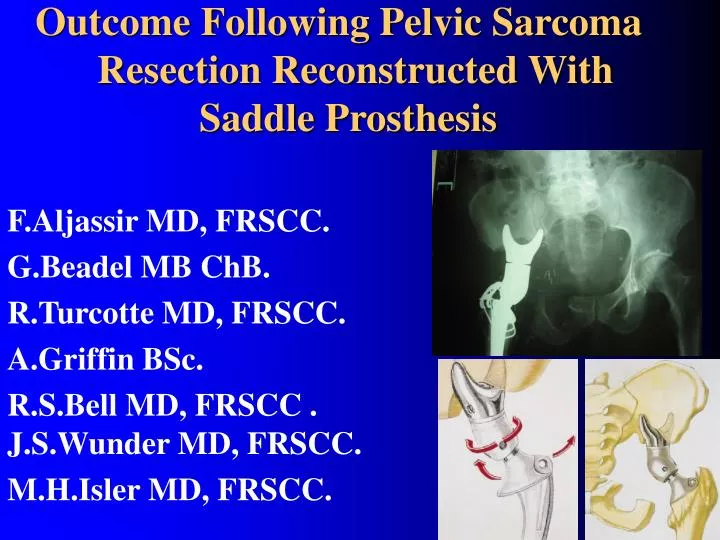
Outcome Following Pelvic Sarcoma Resection Reconstructed With Saddle Prosthesis. F.Aljassir MD, FRSCC. G.Beadel MB ChB. R.Turcotte MD, FRSCC. A.Griffin BSc. R.S.Bell MD, FRSCC . J.S.Wunder MD, FRSCC. M.H.Isler MD, FRSCC. Introduction. Pelvic sarcomas remain a difficult problem.

E N D
Outcome Following Pelvic Sarcoma Resection Reconstructed With Saddle Prosthesis F.Aljassir MD, FRSCC. G.Beadel MB ChB. R.Turcotte MD, FRSCC. A.Griffin BSc. R.S.Bell MD, FRSCC . J.S.Wunder MD, FRSCC. M.H.Isler MD, FRSCC.
Introduction. • Pelvic sarcomas remain a difficult problem. • Classically, hemipelvectomy was the primary means of surgical intervention. • With the advent of aggressive chemotherapy, better imaging studies and more advanced surgical techniques, limb-sparing resections have been increasingly used .
Techniques of surgical reconstruction include: 1-Ischiofemoral arthrodesis or pseudoarthrosis. 2-Iliofemoral arthrodesis or pseudoarthrosis. 3-Massive allograft or autoclaved autograft with hip arthroplasty. 4-Flail extremity. 5-Custom made metallic prostheses. 6-Saddle prosthesis.
The saddle is free to rotate on the body component. The entire prosthesis can abduct, adduct, flex, and extend through the saddle and iliac “articulation”. 3-Saddle 2-body 1-stem
1-Nieder et al(seven:ISOLS, 313, 1993]. - 72 patients (failed of hip arthroplasty). -1 excellent , 14 good , 36 fair , and 21 poor. -Infection in 15 patients lead to poor results. 2-Aboulafia et al: ( Clin Orthop 314:203-213,1995). -17 patients, -mean follow up of (33 mon). -Favorable results: (excellent in 10, good in 2, fair in 1, and poor in 4. In the literatures there are few clinical studies of the saddle prosthesis
3- Windhager et al (Clinical ortho (1996) 331:265-276.) -22 patients (6 had saddle prosthesis) -Custom-made pelvic had better functional results. -Eccentric new hip centre { limited motion}. 4-Renard et al(Arch Orthop Trauma Surg(2000) 120:188-194) -15 patients. -Satisfactory results in short term follow up. 5-Cottias et al(Journal of surgical oncology 2001;78:90-100.) -17 patients, with mean follow up of 42 months -early pain free weight bearing, -minimal limb shortening -functional results remained fair in most patients.
Objectives: • To evaluate the outcome after resection of pelvic sarcoma and reconstruction with a saddle prosthesis.
Material & Methods. • Retrospective study, 27 patients (1991 to 2001). (Maisonneuve- Rosemont Hospital (Montreal) and Mt Sinai Hospital (Toronto). • Functional outcome wasassessed with MSTS 1987 & 1993 and the Toronto Extremity Salvage Score (TESS). • Oncological outcome parameters and complications were recorded.
Patients Demographic • Gender:18 male (67%) / 9 female (33%). • Age: ( 24 to 75 years ) , mean (SD) (53 (16)). • Follow up: ( 12 to 120 months), mean (45 months). • Operative time: ( 300 to 900 minutes ), mean (SD) ( 600 (98 )). • Blood transfusions: from 4 to18 units, mean (SD) (10 (6)).
ChSA OSA MFH EHE mGCT EWSA
TYPE I (ilium) TYPE II (periacetabular) TYPE III (pubis) Enneking WF.The anatomic considerations in tumor surgery: pelvis. In: Enneking WF, editor. Musculoskeletal Tumor Surgery, Vol. 2. New York: Churchill Livingstone.1983: 483–529. Musculoskeletal Cancer Surgery(2001). Martin Malawar
(Enneking WF, Spanier SS, Goodman MA. Asystem for the surgical staging of musculoskeletal sarcoma: Clinical Orthop. 1980 Nov- Dec;(153): 106-20).
Complications. Infection in 10 (37%) 4 were superficial and 6 (22%) were deep. Heterotropic ossification in 10 (37%). post op. One year post op.
Complications. • Dislocations in 6 (22.2%). • Fractures in 6 (22.2%) • Nerve Injuries in 5 (18.5%). • Others (2 dissociations, 3 DVT, and one MI).
Vertical migration 1 2 2 3 4
At mean f/u (45 months). Oncological Outcome. AWD AWOD DCD
At mean f/u (45 months). Oncological Outcome.
Local recurrence in our study: 6/27 (22.2%) 4/6 (67%) had positive resectional margins. Survival rate is (60%) At mean f/u (45 months). Oncological Outcome.
*is similar to other study : 1-mean =17, ( 11to 23). { functional evaluation of 17 Saddle) Cottias et alJournal of surgical oncology 2001; 78:90-100. 2-Mean=17.6, (13 to 26). (endoprosthetic pelvic replacement) Bruns et al(Arch Orthop Trauma Surg(1997)116:27-31). *And lower compare to prox -imal femoral replacement: Mean =23.2 (13 to 33) Ogilivie et alclinical orthopedic and related research 2004;426:44-48 Functional Outcomes. Mean (15)
Custom made prosthetic reconstruction:mean( 70%) Abudu et al ( JBJS Br. 1997;79-B:773-9). • Endoprosthetic pelvic replacement ,(51%). Bruns et al(Arch Orthop Trauma Surg(1997)116:27-31). • Proximal femoral replacement: Mean=67.7% (40-93%) Ogilivie et alclinical orthopedic and related research 2004;426:44-48 Functional Outcomes. Mean (51%)
TESS of limb sparing for lower limb sarcoma (distal thigh): mean (85%) Davis et al, Arch Phys Med Rehabbil. 1999 jun ;80960:615-8. For proximal femoral replacement: Mean = 76% , (40-98) Ogilivie et alclinical orthopedic and related research 2004;426:44-48 Mean = 58%, (39-95) { functional evaluation of 17 Saddle) Cottias et al(Journal of surgical oncology 2001; 78:90-100). Functional Outcomes. Mean (64%)
Work Status: *Full time 5 patients (18.5%). *Early retirement 5 (18.5%). *Disabled 6 (22.2%). *Deceased 11(40.6%). Gait aids: L.L.D: range between 1 and 6 cm, with a mean of 3cm. A cane in 8 patients (30%). Crutches in 5 (18.5%). Walker in 3 patients (11.1%). Shoe lift in 5 patients. A.F.O in 3 patients. Functional Outcome
Discussion. • In pelvic sarcoma goals are to cure the patient and to preserve the best function and quality of life. • Treatment of pelvic sarcoma remains difficult. • Limited data exists to compare functional outcome. • The most common complications are infection and heterotopic ossification.
Conclusion. • Like with other implants, the oncological and functional outcome in limb salvage procedures using a saddle prosthesis remain difficult to predict, and is associated with significant risk of morbidity and complications. • However, the functional results appear to confer an advantage compared to the expected disability following hemipelvectomy.