Download
1 / 2
20 likes | 112 Views
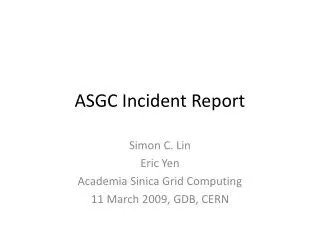
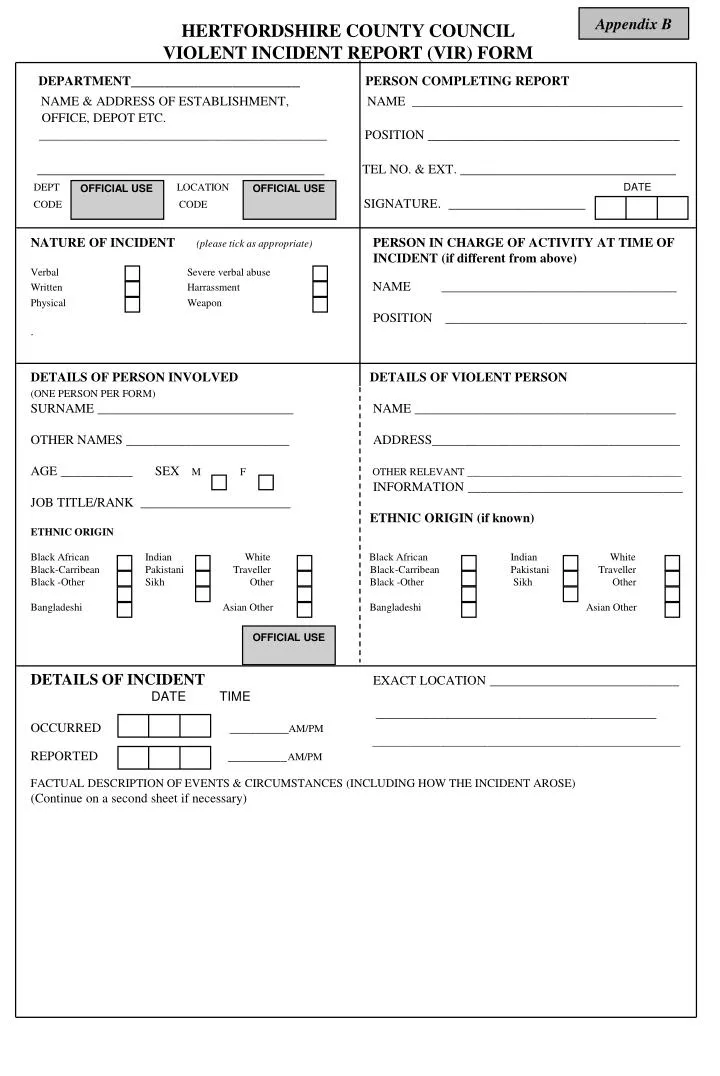
Appendix B. HERTFORDSHIRE COUNTY COUNCIL VIOLENT INCIDENT REPORT (VIR) FORM. DEPARTMENT ____________________ PERSON COMPLETING REPORT NAME & ADDRESS OF ESTABLISHMENT, NAME ______________________________________________

E N D
Appendix B HERTFORDSHIRE COUNTY COUNCIL VIOLENT INCIDENT REPORT (VIR) FORM DEPARTMENT____________________ PERSON COMPLETING REPORT NAME & ADDRESS OF ESTABLISHMENT, NAME ______________________________________________ OFFICE, DEPOT ETC. _________________________________________________ POSITION ___________________________________ ________________________________________ TEL NO. & EXT. ______________________________ DEPT LOCATIONDATE CODE CODE SIGNATURE. ___________________ OFFICIAL USE OFFICIAL USE NATURE OF INCIDENT(please tick as appropriate) PERSON IN CHARGE OF ACTIVITY AT TIME OF INCIDENT (if different from above) Verbal Severe verbal abuse Written Harrassment NAME ____________________________________ Physical Weapon POSITION _____________________________________ . DETAILS OF PERSON INVOLVED DETAILS OF VIOLENT PERSON (ONE PERSON PER FORM) SURNAME ______________________________ NAME ________________________________________ OTHER NAMES _________________________ ADDRESS______________________________________ AGE ___________ SEX M F OTHER RELEVANT _________________________________________ INFORMATION _________________________________ JOB TITLE/RANK _______________________ ETHNIC ORIGIN (if known) ETHNIC ORIGIN Black African Indian White Black African Indian White Black-Carribean Pakistani Traveller Black-Carribean Pakistani Traveller Black -Other Sikh Other Black -Other Sikh Other Bangladeshi Asian Other Bangladeshi Asian Other DETAILS OF INCIDENTEXACT LOCATION _____________________________ DATE TIME _______________________________________ OCCURRED _________AM/PM ___________________________________________________________ REPORTED _________AM/PM FACTUAL DESCRIPTION OF EVENTS & CIRCUMSTANCES (INCLUDING HOW THE INCIDENT AROSE) (Continue on a second sheet if necessary) OFFICIAL USE
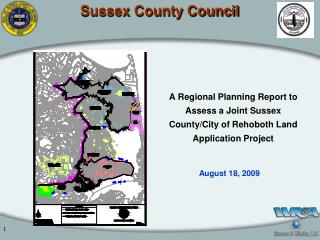
DETAILS OF INJURY AND TREATMENT Was injury sustained? YES NO If YES, give details of nature, site and extent ____________________________________________________________________ ____________________________________________________________________ TYPE OF TREATMENT: HOSPITAL DOCTOR FIRST AID REST NONE DETAILS OF TREATMENT _________________________________________________ OFFICIAL USE OFFICIAL USE OFFICIAL USE NAME & ADDRESS OF HOSPITAL/DOCTOR (If appropriate) WITNESS/ES (continue on separate sheet if necessary) ____________________________________________________ NAME __________________________________ ____________________________________________________ ADDRESS _______________________________ _________________________________________ If an employee, has the injury resulted in absence (ATTACH STATEMENT) from work? YES NO HSE STATUTORY REQUIREMENTS If yes, did he/she do any work on the day of Is incident notifiable to HSE? (See Departmental the incident after it happened? YES NO Safety Arrangements) YES NO IF YES: What time did he/she stop work? _______________am/pm HSE notified by phone? YES NO Anticipated duration of absence _______________ days HSE form F2508 sent? YES NO BY: NAME DATE IF THIS FORM HAS NOT BEEN COMPLETED BY THE MANAGER, MANAGER MUST SIGN HERE TO INDICATE THAT THEY ARE AWARE OF ACCIDENT/INCIDENT DETAILED OVERLEAF AND ABOVE. Manager’s Name: Signature: Date: INVESTIGATION Has the incident been reported to the Police?. YES NO If YES, please give details (including when, where, officer’s names/no’s, action taken) ____________________________________________________________________________________ What was the likely cause of the incident and what would make it less likely to recur? ____________________________________________________________________________________ Give details of any discrepancies found in the information provided and any action taken to investigate and prevent recurrence ____________________________________________________________________________________ _____________________________________________________________________________________________________ Investigating Officer: NAME SIGNATURE POSITION TEL NO. DATE Completion of this form does not constitute a claim against the County Council. NOTE: This form should be completed as soon as possible after the incident and processed in accordance with your departmental arrangements and the original sent to the CSF HEALTH AND SAFETY TEAM, ROOM 159, COUNTY HALL, HERTFORD SG13 8DF