Download
1 / 1
20 likes | 214 Views
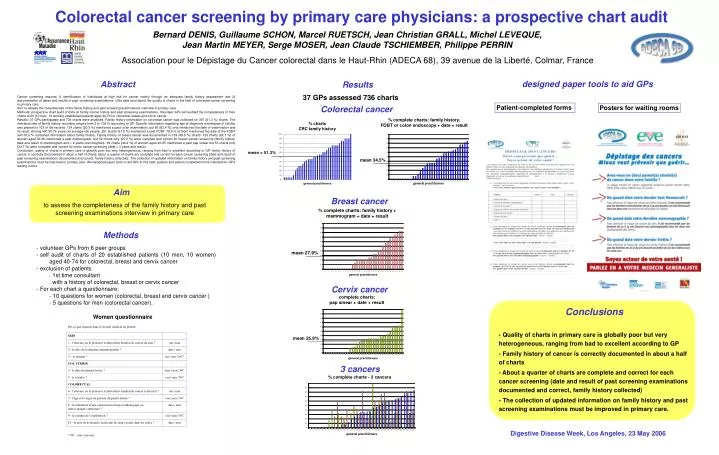
Colorectal cancer screening by primary care physicians: a prospective chart audit. Bernard DENIS, Guillaume SCHON, Marcel RUETSCH, Jean Christian GRALL, Michel LEVEQUE, Jean Martin MEYER, Serge MOSER, Jean Claude TSCHIEMBER, Philippe PERRIN.

E N D
Colorectal cancer screening by primary care physicians: a prospective chart audit Bernard DENIS, Guillaume SCHON, Marcel RUETSCH, Jean Christian GRALL, Michel LEVEQUE, Jean Martin MEYER, Serge MOSER, Jean Claude TSCHIEMBER, Philippe PERRIN Association pour le Dépistage du Cancer colorectal dans le Haut-Rhin (ADECA 68), 39 avenue de la Liberté, Colmar, France designed paper tools to aid GPs Abstract Results 37 GPs assessed 736 charts Cancer screening requires 1) identification of individuals at high risk for cancer mainly through an adequate family history assessment and 2) documentation of dates and results of past screening examinations. Little data exist about the quality of charts in the field of colorectal cancer screening in primary care. Aim: to assess the completeness of the family history and past screening examinations interview in primary care. Methods: prospective chart audit of data on family cancer history and past screening examinations. Volunteer GPs self audited the completeness of their charts of 20 (10 men, 10 women) established patients aged 40-74 for colorectal, breast and cervix cancer. Results: 37 GPs participated and 736 charts were analysed. Family history information on colorectal cancer was collected on 367 (51.3 %) charts. The individual rate of family history recording ranged from 5 to 100 % according to GP. Specific information regarding age at diagnosis and degree of kinship was present in 103 of the records. 134 charts (20.5 %) mentioned a past colon examination, but 85 (63.4 %) only mentioned the date of examination and its result. Among 490 50-74 years old average risk people, 251 charts (51.2 %) mentioned a past FOBT, 78.5 % of them mentioned the date of the FOBT and 63.3 % contained information about family history. Family history of breast cancer was documented in 139 (49.8 %) charts. 126 charts (62.7 %) of women aged 50-69 mentioned a past mammogram, but 52 charts only (25.9 %) were complete and correct for breast cancer screening (family history, date and result of mammogram and < 2 years mammogram). 99 charts (44.2 %) of women aged 40-65 mentioned a past pap smear but 53 charts only (23.7 %) were complete and correct for cervix cancer screening (date < 3 years and result). Conclusion: quality of charts in primary care is globally poor but very heterogeneous, ranging from bad to excellent according to GP: family history of cancer is correctly documented in about a half of charts; about a quarter of charts are complete and correct for each cancer screening (date and result of past screening examinations documented and correct, family history collected). The collection of updated information on family history and past screening examinations must be improved in primary care. We designed paper tools to aid GPs in this task: posters and patient-completed forms intended for GP's waiting rooms. Patient-completed forms Posters for waiting rooms Colorectal cancer Aim Breast cancer to assess the completeness of the family history and past screening examinations interview in primary care Methods • volunteer GPs from 6 peer groups • self audit of charts of 20 established patients (10 men, 10 women) aged 40-74 for colorectal, breast and cervix cancer • exclusion of patients • . 1st time consultant • . with a history of colorectal, breast or cervix cancer • For each chart a questionnaire: • 10 questions for women (colorectal, breast and cervix cancer ) • 5 questions for men (colorectal cancer). Cervix cancer Conclusions - Quality of charts in primary care is globally poor but very heterogeneous, ranging from bad to excellent according to GP - Family history of cancer is correctly documented in about a half of charts - About a quarter of charts are complete and correct for each cancer screening (date and result of past screening examinations documented and correct, family history collected) - The collection of updated information on family history and past screening examinations must be improved in primary care. Women questionnaire 3 cancers Digestive Disease Week, Los Angeles, 23 May 2006