Download
1 / 61
660 likes | 937 Views
Medicolegal Issues in Anatomic Pathology. Mark R. Wick, M.D. Malpractice Claims: Necessities.

E N D
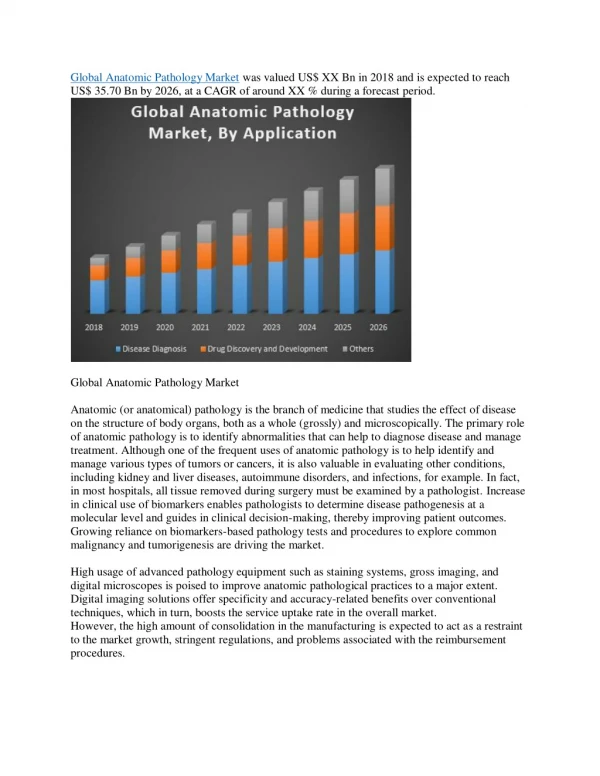
Medicolegal Issues in Anatomic Pathology Mark R. Wick, M.D.
Malpractice Claims: Necessities • Negligence: Defined by “expert” testimony as medical practice that breaches the national or regional standard of care. This is defined as the behavior expected of “prudent, careful, & informed” physician. • Injury: Must be objectively documented and judged to be the direct consequence of the negligent professional action.
Items of Interest Regarding Medical Malpractice Lawsuits • Some states have an institutional cap for damages that is much less than the cap for individual practitioners (e.g., in Virginia the MC cap is ~$100K, whereas the MD cap is $1.6 million) • Selected states allow the plaintiff to file a separate civil action against the personal assets of the physician if there is a malpractice judgment against the doctor (double jeopardy) • The plaintiff’s lawyer is working on a contingency basis– up to 33% of the monetary award to the plaintiff goes to the attorney
Lawsuits Against Pathologists • How likely is it that current practitioners in pathology will be sued during their careers? • Largely dependent upon geographic locale of practice– both coasts, Florida, Texas, Illinois, and selected other cities/counties are “hotbeds” of plaintiff attorney activity • Subspecialty practice area is also important– dermatopathology, cytopathology, & hematopathology are high-profile with regard to lawsuits against pathologists • Most pathologists now in practice will have at least one suit filed against them during their careers
Lawsuits Against Pathologists • Clinically “significant” diagnostic error rate in surgical pathology & cytopathology ranges from 0.25% to ~6% in the published literature • Factors contributing to this situation include a paucity of “hard” diagnostic criteria for many conditions, some variation in individual visual perception and decision-making, and incomplete or misleading clinical information • Despite those realities, the American public & the plaintiff’s bar expect a “zero error standard”
Surgical Pathology Claims Against the Doctors’ Company– 1998-2003[Troxel DB: Am J Surg Pathol 2004; 28: 1092-1095] Specimen Type % Claims %FN %FP Total Claims (%) Breast Bx 42 48 52 15.5 Melanoma 44 95 5 16 Lymphoma 14 57 43 5 FNA, Misc. 10 40 60 3.5 FNA, Breast 5 40 60 2 Gastric biopsy 12 42 58 4.5 Prostate biopsy 9 67 33 3 Lung biopsy 12 42 58 4.5 GYN pathology 31 74 16 11.5 Sarcoma pathology 15 80 20 5.5 Bladder pathology 5 100 0 2 Cysts 3 100 0 1 Miscellaneous 48 65 19 26* _______________________________________________________________________________________________ * Included cases involving failure to diagnose metastatic carcinoma (especially in lymph nodes), suits against primary pathologists for mistakes made by their consultants (“vicarious liability”), failure to solicit consultation or perform special diagnostic studies, frozen section misdiagnoses, and actions resulting from specimen misidentification, processing, or mistakes in written or verbal reporting
Changes in Claims Against Pathologists from 1995 to 2003– Data from The Doctors’ Company • Increased spectrum of claims, with regard to organ systems and diagnoses • Slight decrease in FNA-related claims • Slight increase in melanoma-related claims • New areas of litigation– soft tissue pathology, GYN pathology, bladder pathology, pulmonary pathology
Why are Pathologists Being Increasingly Targeted in Malpractice Suits? • We are, partially, victims of our own success, through efforts of the CAP & ASCP to increase our public visibility • “Because we are out there”… the plaintiff’s bar is always looking to extend its sphere of operations (beyond OB, Anesthesia, ER Medicine, etc.) • The media and other physicians increasingly tell patients that we provide the “final answer” in their cases, and often misrepresent the strengths and weaknesses of pathologic tests & procedures (e.g., in Pap smear cases– c.f. A footnote in “A Case of Need” by Michael Crichton -“The Papp [sic] smear is the most accurate diagnostic test in all of medicine”)
How Do Suits Against Pathologists Usually Happen? • There is a “lag period”--- usually the biological evolution of the case over time, or referral of the patient and his/her pathologic specimens to other centers occasions a change in diagnosis and incites the filing of a suit after legal consultation • The initial pathologist is usually blind-sided; there is rarely a continuous train of information which culminates in the lawsuit • Sometimes the only “fault” of the pathologist is being the person on the signout schedule when a “systems” mistake occurs; e.g., the mislabeling or mixup of a specimen • The pathologist and/or the hospital is served with a written “bill of complaint” from the court, usually necessitating personal delivery from a law enforcement officer • The bill of complaint details the alleged act(s) of malpractice and the supposed consequences to the patient (i.e., the damages)
Consultation with Risk Managers • Virtually all medical centers and medical schools have departments of risk management; these should be contacted immediately if it is thought that a particular case is at risk for a lawsuit. RM personnel would much rather deal with many cases that “never go anywhere” than with problems they know about only after the filing of a bill of complaint • Conversations, meetings, and correspondence with RM personnel are typically regarded as privileged under the law, and the contents thereof are not “discoverable” by plaintiff’s attorneys • Cases with serious procedural irregularities, major changes in diagnosis, or anything inciting anger by the patient (or their family) should be referred to risk managementimmediately • As a general rule, pathologists should never speak to plaintiffs directly after a suit has been threatened or filed, or should do so only after consulting RM regarding known case-related problems Staying Out of Trouble-101
What Should be Done After Receiving a Bill of Complaint (BOC)? • Meet with the attorney representing your hospital or organization, as well as yourself, after sending them the BOC to study • Your lawyer(s) will gather information about the case from you and others, to prepare a written document called a “response”– this is your protestation of innocence of the charges made and is filed with the court and the plaintiff’s attorney • NEVER speak or correspond in any way with the plaintiff’s counsel after the process has begun, except in the presence of your attorney(s)
Things to NEVER Do If You are Afraid of a Lawsuit or Have Already Been Sued Regarding a Specific Case • NEVER talk to other people who have been named in the suit about any details of the case, & certainly never attempt to influence their remembrance of details or events; • NEVER try to alter or discard records, slides, or any other tangible evidence; • NEVER speak or correspond directly with the patients, their family members, or their attorneys about the case; • NEVER try to deflect your own potential culpability by blaming others (“passing the poisoned buck”)– it is unprofessional and hasn’t a prayer of working…
“Life On the Cheap”---Attorneys Trying to Get Something for Nothing • Lawyers will sometimes attempt to bully their way into getting free information by trying to talk with housestaff who are attached to an attending physician being sued, or they will co-name the resident(s) and try to talk with them first (free, of course…); • “Treating physicians” (attending doctors involved in the case but not being sued) will be contacted for a deposition by the plaintiff’s attorney, regarding the defendants’ actions; • ALL physicians being asked legal questions about a case in which they are involved should have their own attorneys present; if they are not named in the suit, they have the right to ask for reimbursement for their time & efforts, and should do so.
The Medical “Expert” or “Authority”—CAUTION! • The meaning of “expert” or “authority” (or “authoritative”) is very different in the law and in common medical parlance • In a legal context, all of these terms imply infallibility– therefore, each word in a textbook or treatise that is deemed “authoritative” is, by definition, unassailably correct • The word “scholarly” is much preferred in verbal or written discourse about medical opinions and publications– it carries no such hidden meaning
Malpractice Suits– Not Scarlet Letters • Physicians who are sued, and who have not committed wrongful acts out of true negligence or personal impairment (e.g., substance abuse) should not take the action personally if at all possible– it is a business proposition for attorneys and nothing more • Personal counseling by a psychiatrist or psychologist is a good idea to work through these concepts and avoid self-recrimination M
Specific Topics & Subspecialty Areas in Pathology Malpractice
ELEMENTS OF HISTOLOGICAL TISSUE PROCESSING THAT CAN RESULT IN LEGAL CLAIMS OF “NEGLIGENCE” • Errors in: • Prosection and fixation of the specimen by the pathologist (or mixup of specimens by persons unknown before receipt in the pathology laboratory) • Automated tissue processing • Paraffin embedding • Microtomy & slide preparation • Histochemical staining • Coverslipping • Interpretation
SOURCES OF TISSUE “FLOATERS” IN MICROSCOPIC SECTIONS THAT CAN RESULT IN MISTAKES IN DIAGNOSIS • “Cutting board” floaters (flawed prosection technique in the gross room) • Automated tissue processor mishaps (transplantation of small tissue fragments from one specimen to another via instrument solutions) • Embedding room mistakes • Poor water bath technique
Illustrative Case: Tissue Processing Mistakes as Sources of a Lawsuit__________________________________________ • A 53 year old woman complained of persistent dyspepsia and was subjected to a gastroesophagoduodenoscopy. The gastroenterologist saw only “mild gastritis,” but obtained several biopsies. These were unexpectedly read as showing enteric-type adenocarcinoma, and a partial gastrectomy was subsequently performed. There was no evidence of malignancy in the resection specimen, despite the fact that the entire mucosal surface was blocked for microscopic examination.
“Floaters” in Surgical Pathology: Potential Sources of Lawsuits Biopsies from gastric biopsy specimen, taken from clinical “mild gastritis” Blood group Ag immunostains done after negative gastrectomy procedure BGB BGA
Illustrative Case: Tissue Sampling Issues as the Source of a Lawsuit__________________________________________ • A 46 year old woman had a needle core breast biopsy in 1995 for a self-detected lesion in the right breast. It was interpreted as showing fibrocystic changes only, and because the mammographer did not have a high level of suspicion for malignancy, nothing further was done. In 1997, the patient presented with right supraclavicular lymphadenopathy, and a lymph node biopsy showed metastatic breast carcinoma (GCDFP-15+/ERP+). The lesion in the right breast was now larger and radiographically atypical, and excision of it showed invasive ductal carcinoma. When recuts of the 1995 biopsy were prepared for referral of the patient to another medical center, a focus of invasive carcinoma was seen that had not been represented in the original set of slides.
Sampling Errors in Preparation of Histologic Slides • Sampling errors in histology can be limited by good laboratory technique, but theycannot be eliminated entirely • Recommendations: • Ask histotechnologists to mount several tissue cuts from small biopsies on each slide, and obtain at least 3 levels of each tissue block • Instruct histotechnologists to be sure to “face into” blocks appropriately • Always have pathologists review any recuts that are prepared on cases being sent away to other institutions, and compare them with the original sections
Education of Histotechnologists on Medicolegal Matters • Plaintiffs’ attorneys are becoming increasingly aware of the details of tissue processing and slide preparation in the histology laboratory • The anonymity of the technologist no longer protects him or her from being the target of a lawsuit, alone or as a “representative” of the medical center • Educational efforts should therefore be directed at histotechnologists in regard to their liability and counter-measures to minimize mistakes and document ongoing quality assurance programs in the laboratory
Hematopathology • Cases concerning failure to diagnose lymphoma principally concern the confusion of follicular lymphoma with lymphoid hyperplasia, and failure to recognize extranodal lymphomas • Confusion between lymphoma/leukemia and EBV or other viral infections and reactive hematolymphoproliferations is also a pitfall in this area • A high index of suspicion is essential in these instances; immunophenotyping and at-least-internal consultation (with documentation thereof in the report) are strongly recommended EBV “LIP”
Illustrative Case: Misdiagnosis of Non-Hodgkin’s Lymphoma___________________________________________________________ • A 41 year old man presented with rapidly-worsening abdominal pain and was found by abdominal MRI scan to have a thickened bowel segment at the ileocecal junction. He underwent laparotomy and resection of the intestine. Because of the presence of transmural chronic inflammation and fibrosis in the bowel wall, a diagnosis of Crohn’s disease was made. Despite treatment with steroids, the patient had recurrent abdominal pain & weight loss and was found 9 months later to have a huge retroperitoneal mass. A biopsy established the diagnosis of large-cell lymphoma, and retrospective review of the original bowel resection disclosed tumor in that specimen as well. The patient died 3 months later.
Resection specimen of ileocecal mass– gross & microscopic images CD20
Where Do Immunostains Stand in Malpractice Actions? • Up until 1999, pathologists were “in limbo” in regard to IHC, because stains were not certified by the FDA for clinical use, and yet they were “state of the art” in actual practice • Now, IHC is indeed considered a necessity of “standard of practice;” it most often enters medicolegal considerations where a lymphoma is misdiagnosed as another form of undifferentiated tumor & the wrong treatment is given subsequently
Dermatopathology • The principal area of liability is that of missed melanoma diagnosis; however, suits have also been filed for overdiagnosis of nevi as forms of melanoma; • Another source of medicolegal action in dermatopathology is the underdiagnosis of squamous cell carcinoma or basal cell carcinoma, with subsequent complications from local tumor growth
Squamous Carcinoma Misinterpreted as Pseudoepitheliomatous Hyperplasia
Illustrative Case: Misdiagnosis of Malignant Melanoma___________________________________________________________ • A 35 year old woman had a 4 cm. irregularly pigmented lesion in the skin of the left leg, for which she consulted a dermatologist. He took a 3 mm. punch biopsy from the periphery of the mass, which was interpreted pathologically as showing a compound nevus. The patient was told she had a benign process and that it need not be excised. When the mass enlarged and began to bleed 11 months later, the patient saw another dermatologist who immediately did a complete excision. That specimen showed an obvious melanoma in vertical growth, with a Breslow depth of 4.1 mm., associated with a compound nevus. The woman subsequently manifested metastases in the brain and died 2 years later. The pathologist was sued but the first dermatologist was not.
Cautionary Notes to Avoid Dermatopathology Missteps • If clinical information indicates that a melanocytic lesion is larger than a biopsy in hand would suggest, make a disclamatory statement in the report which indicates the possibility of sampling error and suggests that excision would be prudent; • If the biology of a melanocytic lesion cannot be determined with certainty, do not try to do so!; • If a keratinocytic proliferation has been only superficially sampled, avoid a definitive interpretation; the term “atypical squamous proliferation” is a good alternative
Breast Biopsies-- Substrates for Malpractice Actions • Sources of legal claims pertaining to breast biopsies: • Failure to ink margins and corresponding inability to comment on them • Failure to provide information on tumor grade, type, size, vascular invasion, surgical margins, hormone receptor status, and associated microscopic findings in the excised breast tissue • Failure to distinguish in the report between in-situ and invasive carcinoma ERP
Synoptic Reporting Forms in Surgical Pathology: Keeping the Wolf from the Door Breast J 2001 Jul-Aug;7(4):271-274 Synoptic/Checklist Reporting of Breast Biopsies: Has the Time Come?Leong ASY.Narrative descriptive reporting has been the traditional format employed in surgical pathology for almost as long as its inception as a specialty. While the descriptive prose has served us well in the past, its accuracy and readability is variable. Descriptions of color, shape, and texture are often subjective. Surgical pathologists are trained observers, but there are inherent differences in reporting style, and descriptive prowess depends on language skills and vocabulary. These differences are reflected in reports generated by pathologists in the same laboratory and may even be more evident in reports from different laboratories and across nations using the English language. The reproducibility of morphologic descriptions is thus a matter of some concern.
FNA Misdiagnoses & Malpractice Suits • The most common site of lesions for which FNA misdiagnosis results in lawsuits is the breast-- this is because surgeons will often perform definitive surgery based principally on the FNA result and may ignore other data; • Sparsely-cellular specimens should not be interpreted with certainty, because of the high rate of false-negative error that attends them; • The most common source of false-positivity is cellular fibroadenoma; hence, if that lesion is in the clinical DDx, the pathologist should be cautious in making a diagnosis of CA
Illustrative Case: FNA Misdiagnosis of Breast Carcinoma___________________________________________________________ • A 37 year old woman palpated a mass in the left breast on self-examination, which was confirmed by her internist. Mammographic examination yielded indeterminate results with respect to the probable malignancy of the lesion, and a consulting surgeon likewise was unsure whether the lesion was carcinomatous or not. An FNA was performed, and a diagnosis of adenocarcinoma was rendered by the pathologist. Based on that information, the surgeon proceeded directly to a simple mastectomy (the woman had small breasts). Surgical pathologic examination of the lesion showed that it was a cellular fibroadenoma. There was no evidence of in-situ or invasive malignancy in the excised breast.
Cautionary Notes Regarding FNA of the Breast • Avoid overinterpretation of sparsely cellular specimens; • ALWAYS seek information on results of physical examination and mammography, before a final cytologic diagnosis is made (the “triple test”); • If there are doubts as to the finality of a diagnosis of carcinoma in the FNA, advise the surgeon to perform a frozen section of the lesion before a definite surgical approach is taken
Illustrative Case: FNA Misdiagnosis of Sarcoma___________________________________________________________ • A 24 year old man had a painless mass in the right Achilles tendon, which had enlarged slowly over a 6 month period. He consulted an orthopedist, who performed a fine needle aspiration biopsy on the lesion. It was interpreted as showing “pigmented villonodular tenosynovitis,” and no further therapy was recommended. Eight months later, the mass was larger still and it was excised, showing a clear-cell sarcoma. Three years thereafter, chest radiographs demonstrated pulmonary metastases.
Non-FNA, Non-GYN Cytology Specimens & Malpractice Suits • Exfoliative pulmonary cytology specimens are relatively high-risk medicolegally, because definitive surgery may be undertaken based upon them; • False-positive results (owing to the effects of infarcts, granulomas, alveolar damage, & other causes) are more damaging than false-negative findings, although the latter are not inconsequential (e.g., failure to make a timely diagnosis of small-cell carcinoma in sputum)
Illustrative Case: Cytological Misdiagnosis of Lung Cancer__________________________________________ • A 56 year old man was found to have a cavitary lesion in the mid-left lung field, in a set of screening chest radiographs. He underwent examination of several sputum cytology specimens, which were negative for malignancy. Subsequently, a bronchoscopy was performed with bronchial brushing and washing. Cytologic specimens from those procedures were interpreted as showing non-small-cell carcinoma. A left pneumonectomy was performed, pathologic examination of which demonstrated only a histoplasmoma with surrounding bronchial atypical squamous metaplasia. There was no evidence of in-situ or invasive malignancy.
Resection specimen (upper left-H&E; upper right- GMS; lower- atypical bronchial epithelial metaplasia)
Intraoperative Followup of Exfoliative Cytologic Diagnosis of Lung Carcinoma • When exfoliative cytology is the only source of a diagnosis of lung cancer, it is wise to prompt the surgeon to ask for a frozen section on the lesion before proceeding with a lobectomy (or more); • Granulomas, infarcts, organizing pneumonias, and other benign processes may yield false-positive cytologic results
The Pap Smear Crisis • In the past 15 years, plaintiffs’ attorneys have discovered Pap smears as a “growth industry,” ignoring the fact that they are screening tests and not intended for definitive diagnosis. The main issue is whether “atypical cells” (no matter how scant) have been missed on smears preceding another one (or a biopsy) that is diagnostic for SIL or invasive SCC. The situation is worsened by the growing presence of several unscrupulous plaintiffs’ “experts” who will testify to virtually anything in this arena.