Download
1 / 67
680 likes | 980 Views
Molecular Pathology of Kidney Diseases. Dr. K.W. Chan. 1. Hereditary Kidney Diseases. Adult polycystic disease Infantile polycystic disease Alport syndrome. 1. Hereditary Kidney Diseases. [Adult polycystic disease] Infantile polycystic disease Alport syndrome. Characteristics of APKD.

E N D
Molecular Pathology ofKidney Diseases Dr. K.W. Chan
1. Hereditary Kidney Diseases Adult polycystic disease Infantile polycystic disease Alport syndrome
1. Hereditary Kidney Diseases [Adult polycystic disease] Infantile polycystic disease Alport syndrome
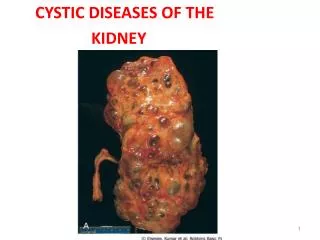
Characteristics of APKD • Gene frequency 1/1000. • Autosomal dominant. • Symptoms onset in middle age. • Large polycystic kidneys. • >50% end stage renal failure. • A disorder affecting multiple organ systems. • Genetically heterogeneous.
Localization of APKD genes • 1986 (Reeders et al) • A gene locus of APKD (now called PKD1) was shown to be closely linked to the -globin locus on 16p. • 1988 (Kimberling) • Genetic heterogeniety of APKD was discovered. • 1992 (Peters et al) • The PKD2 locus was localized to 4q21-23.
1994 (EPKDC) • PKD1 identified to be a gene encoding a 14-kb transcript • encoding a 4,302 a.a. protein called polycystin-1 • 1996 (Mochizuki et al) • PKD2 was cloned and polycystin-2 characterized • 1997 (Ariza et al) • described a 2-generation Spanish family with PKD in which linkage to the PKD1 and PKD2 loci was excluded -> evidence of PKD3
Localization of PKD1 • A Portuguese family with both APKD and TSC • Father normal karyotype • Mother 46,XX t(16;22)(p13.3;q11.21), suffers APKD • Son 45,XY 16pter-p13.3 and 22pter-q11.21, suffers TSC and APKD • The breakpoint at 16p13.3 has disrupted the PKD1
Characteristics of PKD1 • Located on 16p13.3 • ~52kb genomic DNA, 14kb mRNA, 46 exons, 4,302 a.a. • Encodes for polycystin 1, an integral membrane glycoprotein • 70% duplication on 16p13.1 - the HG area • HG-A 21 kb • HG-B 17 kb • HG-C 8.5 kb
Characteristics of PKD2 • Located on 4q21-23. • Encodes a 4 kb mRNA, 968 a.a. product. • Encodes for polycystin 2, an integral membrane glycoprotein. • Polycystin 1 and 2 function together as part of a multi-component membrane-spanning complex involved in cell-cell or cell-matrix interactions.
Polycystin 2 • Polycystin 2 has six transmembrane spans with intracellular amino- and carboxyl-termini. • It has amino acid similarity with PKD1, and the family of voltage-activated calcium (and sodium) channels • It contains a calcium-binding domain.
Aims of genetic study • Early diagnosis, including prenatal and presymptomatic diagnosis. • Select embyro by “test tube baby” • Correlate between phenotype and genotype. • Understand mechanisms involved in cyst formation and other associated lesions of APKD at the molecular level.
Problems in the study of PKD1 • Only about 2.5 kb out of the 14 kb transcript is not duplicated. • Mutations affecting the duplicated part are difficult to determine. • No “hot spot” mutations.
Diagnosis by Imaging • Ultrasonography • Intravenous urography • Urogram with bolus intravenous nephrotomography • Computerized tomography
Age No. of cysts Remarks < 30 2 Unilateral / Bilateral 30 – 59 2 In each kidney > 60 > 3 In each kidney Diagnostic Criteria of APKD
Strategies for genetic study • Genetic linkage study for early diagnosis • Microsatellite studies in APKD kindreds • Mutation analysis • Sequencing • Only about 2.5 kb out of the 14 kb transcript is not duplicated. • Mutations affecting the duplicated part are difficult to determine. • No “hot spot” mutations.
Microsatellite Polymorphism • Variation in the number of dinucleotides within (AC)n or other simple sequence repeats
Scope of work • Characterization of markers in HK Population (a sample of 63 unrelated adults) • 6 PKD1 markers, 3 PKD2 markers • Microsatellite haplotyping in 5 APKD families with a total of 42 members.
Method • 20 ml of peripheral blood • DNA extracted and purified • PCR amplification of each of the 9 microsatellite markers • Southern blot
Marker No. of subjects Type of Allele HET PIC SM7 57 9 0.639 0.609 CW2 46 7 0.789 0.760 AC2.5 54 9 0.754 0.720 SM6 54 14 0.652 0.635 KG8 56 4 0.246 0.229 D16S521 51 11 0.639 0.609 D4S231 52 10 0.840 0.807 D4S1563 57 7 0.775 0.741 D4S414 54 9 0.823 0.793 Microsatellite Characterization
PKD1 Markers in Family D (SM7) (SM6) IIa IIa IIb IIb IIc IIc Ia Ia Ib Ib Z,Z Z,Z Z,Z+4 Z,Z+4 Z,Z+4 Z,Z+6 Z,Z+4 Z+2,Z+4 Z+4,Z+6 Z+2,Z+6 (CW2) (KG8) Z,Z Z,Z Z,Z Z-1,Z Z,Z+1 Z,Z+2 Z,Z+2 Z,Z+2 Z-1,Z+2 Z-1,Z+1 (AC2.5) (D16S521) Z,Z Z,Z Z,Z Z,Z+6 Z,Z+5 Z,Z+4 Z,Z+4 Z,Z+4 Z,Z+5 Z+5,Z+6
PKD1 Markers in family E (SM7) (SM6) Ic Ic IIb IIb IIa IIa Ib Ib Ia Ia Z,Z Z,Z Z-4,Z Z-9,Z Z,Z+4 Z-5,Z Z-9,Z Z-4,Z+2 Z-4,Z+6 Z,Z+6 (CW2) (KG8) Z,Z Z,Z Z-3,Z Z-2,Z Z-2,Z Z-2,Z Z-2,Z Z-2,Z-1 Z-3,Z-2 Z-3,Z+1 (AC2.5) (D16S521) Z,Z Z,Z Z,Z Z,Z+2 Z,Z+6 Z,Z+6 Z,Z+6 Z,Z+6 Z,Z+6 Z+6,Z+7
Family Generation No. of Member ADPKD1 ADPKD2 A 2 6 + - B 2 8 ++ -- C 3 18 +++ -- D 2 5 - - E 2 5 ND ND Results of Genetic Diagnosis
PKD3 - Is there one? • 2001 (Pei et al) • evidence of bilineal disease and trans-heterozygotes in a large family of ADPKD • 28/48 members affected • SSCA screened for and found a PKD2 mutation (2152delA; L736X) in 12 affected pedigree members • linkage analysis with markers at the PKD1 locus, found significant LOD scores (13.0).
PKD3 - Is there one? • 2001 (Pei et al) • evidence of bilineal disease and trans-heterozygotes in a large family of ADPKD • 28/48 members affected • in 2/48, who had severe disease, evidence of trans-heterozygotes
1. Hereditary Kidney Diseases Adult Polycystic Disease [Infantile Polycystic Disease] Alport Syndrome
Infantile Polycystic Kidney Disease • Autosomal recessive. • Usually incompatible with life. • Early antenatal diagnosis for termination of pregnancy is desirable.
Infantile Polycystic Disease • In infantile PKD, the liver is always affected. • The abnormal bile ducts in the liver are accompanied by periductal fibrosis. Hence called congenital hepatic fibrosis.
Localization of PKHD1 • 1994 • Gene locus in 6p12.1-p21. • 2002 (Ward et al) • PKHD1 cloned • 16kb transcript, 4,074 a.a. receptor-like protein called fibrocystin • Missense and truncating mutationsidentified in 14 probands
Genetics of PKHD • Compound heterozygosity. • Double truncating mutations – severe disease. • Some families with mild disease show compound heterozygosity for a missense and a truncating mutation.
1. Hereditary Kidney Diseases Adult Polycystic Disease Infantile Polycystic Disease [Alport Syndrome]
Alport Syndrome • A hereditary disorder of basement membrane collagen characterized clinically by hematuria, progressive renal failure, and, frequently, neurosensory hearing loss and ocular abnormalities.
Alport Syndrome • Genetically heterogeneous. • In the majority of cases, the disease is inherited as an X-linked trait, but an autosomal recessive form and also an autosomal dominant form exist.
Alport Syndrome • X-link recessive: mutations of COL4A5 on Xq22. • X-link recessive associated with diffuse leiomyomatosis: mutations of COL4A5 and COL4A6. • Autosomal recessive: mutations of COL4A3 and COL4A4 on 2q. • Autosomal dominant : no mutation in any of the COL4 genes.
Prenatal Diagnosis of AS • X-link recessive: by genetic linkage analysis using polymorphic markers in and around COL4A5. • Autosomal recessive: by genetic linkage analysis using polymorphic markers in and around COL4A3 and COL4A4.
Fabry disease The story begins…
Fabry disease • X-linked recessive inborn error of glycosphingolipid catabolism that results from the deficient activity of the lysosomal enzyme α-galactosidase A (EC 3.2.1.22). • Accumulation of glycosphingolipid substrates in the vascular endothelium causing occlusive microvascular diseases mainly affecting the kidney, the heart, peripheral nerves and the brain.
F/50 Southern Chinese • Asymptomatic proteinuria • 24 hour urine protein 0.6 g • No skin or corneal lesions • Normal renal function tests
Family history • Mother died of kidney disease • 4 siblings • one younger brother (age 44) in end stage renal failure since age of 35 • one younger brother (age 41) has cardiomyopathy since age of 33, not in renal failure
Renal Biopsy Diagnosis • Consistent with heterozygous Fabry disease
Diagnosis Confirmed • Consistent withheterozygous Fabry disease • Low serum α-galactosidase A activity at 5.2nmol/ml.hr • (normal range: 8.8-14.5nmol/ml.hr) • Low serum α-galactosidase A activity in both brothers (both at <0.5nmol/ml.hr)