Download
1 / 103
1.19k likes | 2.07k Views
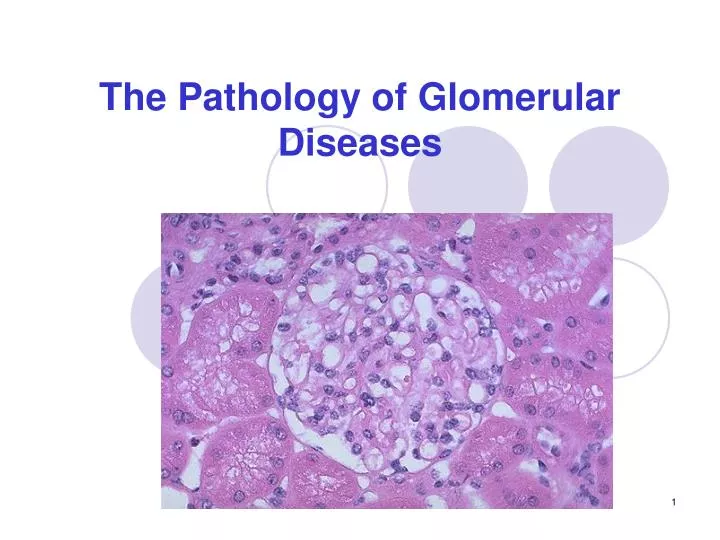
The Pathology of Glomerular Diseases. Pelvis, Cortex, medulla, calyces Renal Artery. - The glomerulus is essentially a tuft of around 50 capillaries, each of which is a unit of the filter. - They are surrounded by Bowman's capsule which encloses the urinary space. Glomerulus.

E N D
Pelvis, Cortex, medulla, calyces • Renal Artery
- The glomerulus is essentially a tuft of around 50 capillaries, each of which is a unit of the filter. - They are surrounded by Bowman's capsule which encloses the urinary space.
Glomerulus Capillary loops Juxtaglomerular apparatus DCT Afferent Arteriole Efferent
Glomerular capillary pericytes are called mesangial cells. • These produce mesangial matrix, which is the supporting framework for the GBM and is chemically the same. • Mesangial cells are contractile, helping regulate flow and filtration rate in the glomerular tuft Glomerular structure
Bowman's capsule encloses the "urinary space" and is continuous with the proximal convoluted tubule.
1700 L of blood filtered 180 L of Glomerul filtrate 1.5 L of urine / day.
1. Fenestrated Endothelium 2. Lamina Rara Interna 3. Lamina Rara Densa 4. Lamina Rara Externa 5. Podocytes + Slit membrane Glomerular Filtration CapillaryLumen
Glomerular Filtration BLOOD Glomerular Capillary Lumen Lamina rara interna Lamina densa Lamina rara externa Foot Processes Podocyte (Visceral epithelium) GBM + FILTRATE Bowman’s Capsule Space
What does kidney do? • Excretes the waste products of metabolism • Regulates the body's content of water, sodium, and potassium. • Maintains the appropriate acid-base balance of plasma • Makes renin and erythropoietin • Activates vitamin D
Primary Glomerular diseases Minor Glomerular abnormalities: Minimal Change disease Focal and/or segmental lesions: Focal glomerulosclerosis Focal proliferative glomerulonephritis Diffuse glomerulonephritis Chronic GN (Irreversible and most common cause of CRF) Glomerulopathies in Systemic diseases SLE Diabetes mellitus Goodpasture Bacterial endocarditis Amyloidosis Vascular disorders Hypertension PAN Wegener’s granulomatosis Henoch-Schönlein purpura. Glomerular diseases
Immune Glomerulonephritis • Antigen or Antibody or immune complex deposition. • Immune reaction • Activation of complement system • Destruction of glomerular structure • Inflammation • Affect renal function
In situ immune complex deposition • Tissue antigens - Masugi / Goodpasture anti GBM Ag • Planted antigens - Heymann / infections, toxins, drugs • Circulating immune complex deposition • Endogenous - SLE • Exogenous - infections (streptococci) Immune Complex ANTI-GBM HEYMANN
Classification of Glomerular diseases • Clinical manifestations (by clinicians) • nephritic syndrome • nephrotic syndrome • RPGN • hemolytic-uremic syndrome • asymptomatic hematuria • Mechanisms of glomerular injury (by immunologists) • anti-GBM disease, • mesangial IgA disease, etc.
DIAGNOSTIC FEATURES OF • GLOMERULAR DISEASES • Light microscopy • Cellularity • Extracellular matrix • Special stains • (PAS, amyloid) • Immunofluorescence microscopy • (Linear, granular, mesangial, irregular deposits) • Electron microscopy • (deposits of immune complexes, BM changes, amyloid)
Histologic and ultrastructural appearance of injury (by light and electron microscopy) • diffuse (all glomeruli) • focal (only some glomeruli, maybe under 80%) • focal-segmental (some glomeruli-some part) • segmental (a part of a glomerulus) • global (entire glomerulus) • proliferative (hypercellular) • necrotizing (necrotizing) • sclerosing (increase in basement membrane - mesangial matrix material)
Histopathologic findings • Cellular proliferation • Endothelial • Mesangial • Epithelial Endocapillary Extracapillary /Crescent formation • Leukocytic infiltration • Glomerular basement membrane thickening • Hyalinization and sclerosis • Electron-dense deposits
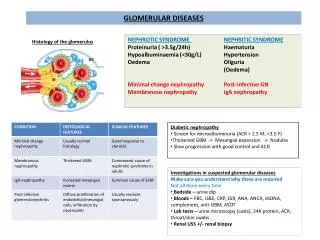
Clinical Syndromes • Nephritic syndrome (nephritis) • Oliguria (GFR, Cr, BUN), Hematuria, Proteinuria, Hypoalbuminemia, Edema (salt and water retention), Hypertension • Nephrotic syndrome • Heavy proteinuria (>3.5 g/24 Hours), Hypoalbuminemia, Severe edema, Hyperlipidemia, Lipiduria, Hypotension • Acute renal failure (RPGN) • Oliguria, loss of Kidney functions - within weeks • Chronic renal failure • Over months and years - Uremia
Clinical-Pathological Correlations • Almost any variety of histopathologic findings can be found in any of the clinical syndromes and vice versa • There are broad correspondences between prognosis and histologic findings. • Each morphologic type of glomerular disease has a clinic correlation as well as etiology and pathogenesis.
Glomerulonephritis: • Immune mechanisms – Most common • Toxins - poisoning • Metabolic – acidosis, hemolysis, etc. • Activation of complement system • destruction of glomerular structure • Inflammation • Affect renal function – excess filtration or decreased filtration. (with RBC & WBC)
Histological Classification of Primary Glomerular Diseases • Minor Glomerular abnormalities: Minimal Change disease • Focal and/or segmental lesions: Focal glomerulosclerosis Focal proliferative GN • Diffuse glomerulonephritis: Mesangial proliferative GN Endocapillary proliferative GN Extracapillary proliferative GN (crescentic GN) Membranoproliferative GN *Type I-II-III • Chronic Glomerulonephritis (Irreversible and most common cause of CRF)
Minimal Change Disease • MINIMAL CHANGE GLOMERULOPATHY ("minimal change disease", "foot process disease", "lipoid nephrosis", "nil lesion", "nil disease") • The most common cause of the nephrotic syndrome in children (peak 2-3 years old) • Adults may be affected: in some of Hodgkin's Disease, Non-Hodgkin Lymphoma and Renal cell carcinoma patients
Electron microscopy reveals diffuse effecement (fusion) of foot processes of epithelial cells. • There is no evidence of immunologic disturbance by immunflourescence microscopy, and the glomeruli appear normal by light microscopy. • Proximal tubules may contain fine lipid droplets. • The most important clinical aspect of minimal change disease is: its good response to steroids!
Minimal Change Disease Loss of Foot processes
Focal and Segmental Lesions Focal glomerulosclerosis (FSGS) (Focal and segmental glomerulosclerosis with hyalinosis, focal sclerosis, Focal sclerosing glomerulonephritis, focal sclerosing glomerulopathy) The term focal glomerulosclerosis is used to describe a morphologic entity characterized by a sclerotic process involving only a portion of the glomeruli and among the affected glomeruli, only a portion of the glomerular tuft. 1-Idiopathic FSGS 2-FSGS superimposed on another primary glomerulopathy, 3-FSGS associated with loss of renal mass 4- Secondary FSGS associated with other known disorders (Heroin abuse, HIV infection)
Microscopic study shows diffuse loss of foot processes (as in minimal change disease) plus focal-segmental sclerosis • There is always striking hyaline arteriolar sclerosis.
Focal Segmental Glomerulosclerosis Hyaline arteriolosclerosis
Idiopathic FSGS poor response to steroids Accounts 10-15% of the cases of nephrotic synd. seen among adults and children. They differ from minimal change disease in the following aspects: 1- They have a higher incidence to hematuria, reduced GFR and hypertension 2- Proteinuria is non-selective 3- IF shows deposition of IgM and C3 in sclerotic segments. 4- Most of them will progress to CRF 5- There is a high reccurrence risk of FSGS in transplant receipents!
HIV associated FSGS Occurs in 5% of HIV infected patients. Light microscopy shows: segmental sclerosis, Capillary collapse, accumulation of hyaline subendothelial deposits and lipid. Electrone microscopy (em) shows tubuloreticular inclusions in endothelial cells. This finding is highly suspective for HIV infection! Clinical presentation is generally Nephrotic syndrome! But some of the patients may have asymptomatic proteinuria and hematuria. Serum complement components are normal.
Focal and segmental Proliferative Glomerulonephritis Represents histologic entity in which glomerular proliferation is restricted to segments or a certain proportion of glomeruli. Focal necrosis or fibrin deposition may occur. These lesions should be differentiated from focal sclerosis.
Focal glomerulonephritis occurs under 3 circumstances: 1-It may be an early or mild manifestation of systemic disease such as SLE, PAN, Goodpasture Synd., Wegener’s granulomatosis. 2- It may be a component of a known glomerular disease such as IgA nephropathy. 3- It may also occur unrelated to any systemic disease and constitute a form of primary focal GN. In this case, clinical manifestations may be in form of hematuria or proteinuria. The prognosis and therapy depends on the underlying disorder.
IgA nephropathy • Berger's disease, idiopathic IgA nephropathy • Most common serious glomerular disease (15-30 years). • IgA nephropathy has a variable prognosis • Mesangial and focal-segmental proliferation and sclerosis may be seen by light microscopy. In bad cases, crescents develop. • Immunofluorescence shows IgA deposited in the mesangium (often with IgG, IgM, and/or C3, but no C4, i.e., the alternate pathway of complement is being activated.)
There are also secondary forms of IgA nephropathy which occur in patients with liver and intestinal diseases. • IgA nephropathy is related to Henoch-Schonlein purpura. • The clinical course is generally benign and slowly progressive. • 50% of patients progress to RF over a period of 20 years. • Older age at onset, heavy proteinuria, hypertension, and presence of crescents are poor prognostic factors. • IgA deposition reccurs in 50% of transplanted kidneys.
Diffuse Glomerulonephritis: • Mesengial proliferative GN • Endocapillary proliferative GN • Extracapillary proliferative GN • Membranoproliferative GN (Type I,II and III) • Membranous GN
Mesengial proliferative Glomerulonephritis • Proliferation of cells in mesengial matrix in the mesangium without involvement of capillary walls or lumina is a non-specific process that occurs in a variety of renal diseases from Lupus nephritis, Resolving post-streptococcal GN, IgA nephropathy and familial nephritis. • This lesion is uncommon in adults over 40 • Causes 5-10% of nephrotic Syndrome in Children. • Prognosis depends on the etiology.
Endocapillary Proliferative Glomerulonephritis (Acute diffuse proliferative and exudative GN.) • Post-Streptococcal GN is prototype for this lesion. Although the disease is mostly seen after infection with streptococci (Nephritogenic strains, types 12, 4, and 1) it also occurs sporadically in association with other bacterial infections, such as staphylococci and pneumococci. • A number of viral infections such as HBV, varicella and Infectious Mononucleosis may also be followed by a similar course. • The term post-infectious GN is also used for this entity.
The cause is deposition of circulating immune complexes which fix complement and attract PMN's (Streptococcal antigens also activate properdin) • Granular deposits of IgG,IgM & C3 in GBM(subepithelial location is common) • Humps in GBM on EM or IF Microscopy (Lumpy-bumpy deposits)
Normal Proliferative
Diffuse Endocapillary Proliferative GN • Proliferation of endothelial and mesangial cells • Cell Swelling • Inflammatory cells (PMNL) • Obstruction ofcapillary lumina • Enlarged hypercellular glomeruli.
Immunofluorescence shows coarse granular deposits containing immunoglobulin and complement. Diffuse Endocapillary Proliferative GN
Prognosis is generally good in children • Over 95% of children recover totally. • Only 1% of children may develop rapidly progressive form or may undergo slow progression to Chronic GN • In adults prognosis is less benign. • 60% of adults may recover from the disease. • The morphologic picture of diffuse endocapillary proliferative GN may also be seen in systemic diseases such as SLE. Prognosis and therapy in these instances will depend on the underlying disorder.
Extracapillary proliferative Glomerulonephritis (Crescentic GN, Rapidly progressive glomerulonephritis-RPGN) This form of GN represents a clinicopathologic syndrome in which rapid and progressive decline in renal function is associated with severe oliguria and anuria, usually resulting in irreversible renal failure in weeks or months. It is characterized by extensive proliferation of the cells in the Bowman’s space with conspicious crescent formation. Hematuria is a common finding, but proteinuria or hyprtension and edema may or may not be present.
Crescentic GN may occur in course of several disorders: • Post-infectious crescentic GN • GN associated with systemic diseases including SLE, Goodpasture, PAN, Wegener’s granulomatosis, Henoch Schonlein purpura, Cryoglobulinemic GN. • Idiopathic (pauci-immune) crescentic GN.