Download
1 / 1
10 likes | 280 Views
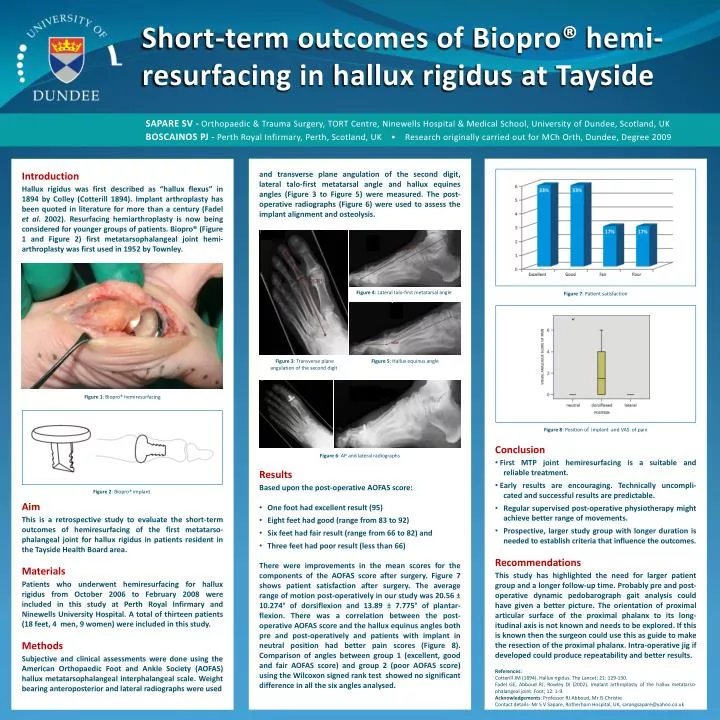
Short-term outcomes of Biopro ® hemi-resurfacing in hallux rigidus at Tayside. SAPARE SV - Orthopaedic & Trauma Surgery, TORT Centre, Ninewells Hospital & Medical School, University of Dundee, Scotland, UK

E N D
Short-term outcomes of Biopro® hemi-resurfacing in halluxrigidus at Tayside • SAPARE SV - Orthopaedic & Trauma Surgery, TORT Centre, Ninewells Hospital & Medical School, University of Dundee, Scotland, UK • BOSCAINOS PJ - Perth Royal Infirmary, Perth, Scotland, UK • Research originally carried out for MCh Orth, Dundee, Degree 2009 • and transverse plane angulation of the second digit, lateral talo-first metatarsal angle and hallux equines angles (Figure 3 to Figure 5) were measured. The post-operative radiographs (Figure 6) were used to assess the implant alignment and osteolysis. • Figure 4: Lateral talo-first metatarsal angle • Figure 3: Transverse plane Figure 5: Halluxequinus angle • angulation of the second digit • Figure 6: AP and lateral radiographs • Results • Based upon the post-operative AOFAS score: • One foot had excellent result (95) • Eight feet had good (range from 83 to 92) • Six feet had fair result (range from 66 to 82) and • Three feet had poor result (less than 66) • There were improvements in the mean scores for the components of the AOFAS score after surgery. Figure 7 shows patient satisfaction after surgery. The average range of motion post-operatively in our study was 20.56 ± 10.274° of dorsiflexion and 13.89 ± 7.775° of plantar-flexion. There was a correlation between the post-operative AOFAS score and the halluxequinus angles both pre and post-operatively and patients with implant in neutral position had better pain scores (Figure 8). Comparison of angles between group 1 (excellent, good and fair AOFAS score) and group 2 (poor AOFAS score) using the Wilcoxon signed rank test showed no significant difference in all the six angles analysed. • Figure 7: Patient satisfaction • Figure 8: Position of implant and VAS of pain • Conclusion • First MTP joint hemiresurfacing is a suitable and reliable treatment. • Early results are encouraging. Technically uncompli- cated and successful results are predictable. • Regular supervised post-operative physiotherapy might achieve better range of movements. • Prospective, larger study group with longer duration is needed to establish criteria that influence the outcomes. • Recommendations • This study has highlighted the need for larger patient group and a longer follow-up time. Probably pre and post-operative dynamic pedobarograph gait analysis could have given a better picture. The orientation of proximal articular surface of the proximal phalanx to its long-itudinal axis is not known and needs to be explored. If this is known then the surgeon could use this as guide to make the resection of the proximal phalanx. Intra-operative jig if developed could produce repeatability and better results. • References: • Cotterill JM (1894). Halluxrigidus. The Lancet; 21: 129-130. • Fadel GE, Abboud RJ, Rowley DI (2002). Implant arthroplasty of the halluxmetatarso-phalangeal joint. Foot; 12: 1-9. • Acknowledgements: Professor RJ Abboud, Mr IS Christie • Contact details- Mr S V Sapare, Rotherham Hospital, UK, sarangsapare@yahoo.co.uk Introduction Hallux rigidus was first described as “hallux flexus” in 1894 by Colley (Cotterill 1894). Implant arthroplasty has been quoted in literature for more than a century (Fadel et al. 2002). Resurfacing hemiarthroplasty is now being considered for younger groups of patients. Biopro® (Figure 1 and Figure 2) first metatarsophalangeal joint hemi-arthroplasty was first used in 1952 by Townley. Figure 1: Biopro® hemiresurfacing Figure 2: Biopro® implant. Aim This is a retrospective study to evaluate the short-term outcomes of hemiresurfacing of the first metatarso-phalangeal joint for hallux rigidus in patients resident in the Tayside Health Board area. Materials Patients who underwent hemiresurfacing for hallux rigidus from October 2006 to February 2008 were included in this study at Perth Royal Infirmary and Ninewells University Hospital. A total of thirteen patients (18 feet, 4 men, 9 women) were included in this study. Methods Subjective and clinical assessments were done using the American Orthopaedic Foot and Ankle Society (AOFAS) hallux metatarsophalangealinterphalangeal scale. Weight bearing anteroposterior and lateral radiographs were used