Download
1 / 28
400 likes | 967 Views
TRAUMATIC SPINAL CORD INJURY. IMPLIES TRAUMA AS THE CAUSE RATHER THAN MEDICAL CONDITIONS [HAVE INCLUDED SOME OTHER ‘SURGICAL CONDITIONS’]. LIFE CHANGING INJURIES. HISTORICAL VIEW. THERE ARE FEW MORE DEVASTATING INJURIES. TENDS TO EFFECT YOUNG PEOPLE etc..

E N D
TRAUMATIC SPINAL CORD INJURY IMPLIES TRAUMA AS THE CAUSE RATHER THAN MEDICAL CONDITIONS [HAVE INCLUDED SOME OTHER ‘SURGICAL CONDITIONS’] SPINEWORKS
LIFE CHANGING INJURIES SPINEWORKS
HISTORICAL VIEW • THERE ARE FEW MORE DEVASTATING INJURIES. TENDS TO EFFECT YOUNG PEOPLE etc.. • ‘THE FROG DIES INSTANTLY WHEN THE SPINAL CORD IS PIERCED; AND PREVIOUS TO THIS IT LIVED WITHOUT HEAD, WITHOUT HEART OR ANY BOWELS OR INTESTINE OR SKIN; AND THEREFORE IT WOULD SEEM LIES THE FOUNDATION OF MOVEMENT AND LIFE’. LEONARDO DA VINCI SPINEWORKS
HISTORICAL VIEW • DESCRIBED IN ANCIENT GREECE IN 2500BC. • KNOWN TO HIPPOCRATES AND HE ATTEMPTS TO REDUCE SPINAL DEFORMITY. • AULUS CELSUS 30BC NOTES THE EFFECTS OF INJURY TO THE SPINAL CORD • GALEN 150BC GREATEST CONTRIBUTION • IN 1824 CHARLES BELL STATES: ‘LAYING A PATIENT UPON HIS BELLY AND BY INCISIONS LAYING BARE THE BONES OF THE SPINE, BREAKING UP THESE BONES AND EXPOSING THE SPINAL MARROW ITSELF, EXCEEDS ALL BELIEF!’ SPINEWORKS
HISTORICAL VIEW • DR ALBAN SMITH IN KENTUCKY PERFORMS THE FIRST SUCCESSFUL LAMINECTOMY FOR TRAUMA IN 1829. • LATER DEVELOPMENTS IN SURGERY NOW MAKE IT MORE ACCEPTABLE. • LATER DEVELOPMENTS FOCUS ON PROMOTING NEUROLOGICAL RECOVERY SPINEWORKS
INCIDENCE • 10,000 NEW SPINAL CORD INJURY PATIENTS / YEAR USA. 15 – 40 / MILLION WORLD WIDE. • THORACIC [T4 – T9] SCI LEAST CHANCE OF IMPROVEMENT. • THORACO-LUMBAR [T10 – T12] MORE CHANCE. ? MORE LOWER MOTOR NEURONES. SPINEWORKS
PHASES • IMMEDIATE - < 2 HOURS • EARLY ACUTE - < 48 HOURS • SUBACUTE - < 14 DAYS • INTERMEDIATE - < 6 MONTHS • CHRONIC - > 6 MONTHS SPINEWORKS
IMMEDIATE • COMPRESSIVE / CONTUSIVE INJURY = MOST COMMON • IMMEDIATE TRAUMATIC INJURY AND SUSTAINED COMPRESSION • MECHANISMS = SHEARING, LACERATION, ACUTE STRETCHING, SUDDEN ACCELERATION / DECCELERATION. • IMMEDIATE TREATMENT = STABILISE, REDUCE COMPRESSION AND SWELLING. SPINEWORKS
SECONDARY INJURY • CONTINUING HAEMHORRAGE • INCREASING OEDEMA AND INFLAMMATION • DUE TO MICROVASCULAR DISRUPTION LEADING TO ISCHAEMIA AND CELL DEATH. • INFLAMMATORY RESPONSE: SOME PARTS BENEFICIAL SOME DELETERIOUS • RESEARCH ON CELL REPAIR SPINEWORKS
DEATH WITH SCI • ADVANCED AGE • HIGH CORD INJURY • INFECTIONS • P.E. • MEDICAL CO-MORBIDITY • SUICIDE • RATE IS ABOUT 4.4% - 16.7% SPINEWORKS
CONSIDERATIONS • PARALYSIS • CAUDA EQUINA SYNDROME • TRAUMATIC CENTRAL CORD SYNDROME • NERVE ROOT COMPRESSIONS SPINEWORKS
AMERICAN SPINAL INJURY ASSOCIATION [FRANKEL] • A = COMPLETE: NO MOTOR OR SENSORY FUNCTION IS PRESERVED IN THE SACRAL SEGMENTS S4-S5.B = INCOMPLETE: SENSORY BUT NOT MOTOR FUNCTION IS PRESERVED BELOW THE NEUROLOGICAL LEVEL AND INCLUDES THE SACRAL SEGMENTS S4-S5.C = INCOMPLETE: MOTOR FUNCTION IS PRESERVED BELOW THE NEUROLOGICAL LEVEL, AND MORE THAN HALF OF KEY MUSCLES BELOW THE NEUROLOGICAL LEVEL HAVE A MUSCLE GRADE LESS THAN 3.D = INCOMPLETE: MOTOR FUNCTION IS PRESERVED BELOW THE NEUROLOGICAL LEVEL, AND AT LEAST HALF OF KEY MUSCLES BELOW THE NEUROLOGICAL LEVEL HAVE A MUSCLE GRADE OF 3 OR MORE.E = NORMAL: MOTOR AND SENSORY FUNCTION ARE NORMAL. SPINEWORKS
DIAGNOSIS IN PARALYSIS • ESTABLISH CAUSE • CORRECT IMAGING • EXTENSIVE NEUROLOGICAL EXAMINATION • POSSIBLE TREATMENT? • MEDICAL • SURGICAL SPINEWORKS
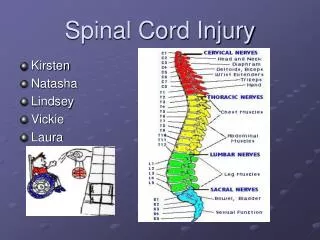
SPINAL CORD INJURY SPINEWORKS
AUTONOMIC FUNCTION ASSESSMENT SPINEWORKS
EXTENT OF SCI SPINEWORKS
ACUTE MEDICAL TREATMENT OF S.C.I. • USE OF STEROIDS CAN BE BENEFICIAL BUT NEED TO BE STARTED WITHIN 8 HOURS AND CONTINUED FOR 48 HOURS. • ANTIBIOTICS IN CORD COMPRESSION FROM ABSCESSES SPINEWORKS
SURGICAL MANAGEMENT • DECOMPRESSION / STABILISATION • TUMOURS • FRACTURES • ABSCESS • DISC HERNIATION • IATROGENIC SPINEWORKS
IATROGENIC • OCCURS DURING SURGERY • VASCULAR INJURY • SCOLIOSIS • THORACIC OR ABDOMINAL AORTA • DISC SURGERY / DECOMPRESSION • POST OPERATIVE HAEMHORRAGE SPINEWORKS
SURGICAL PATHOLOGY SPINEWORKS
HARDWARE SPINEWORKS
SURGICAL MANAGEMENT STABILISATION • IN TANDEM WITH DECOMPRESSION • TO STABILISE IN ESTABLISHED PARALYSIS SPINEWORKS
CAUDA EQUINA SYNDROME • DEFINITIONS • MEDICAL TREATMENT [ABSCESSES, INFLAMATORY CONDITIONS] • SURGICAL TREATMENT [ DECOMPRESSIONS / DISCECTOMY] LOW BACK PAIN, OFTEN VERY SEVERE. THIS IS NOT REGULAR BACK PAIN. SCIATICA IN ONE OR BOTH LEGS, AGAIN USUALLY SEVERE. LEG MUSCLE WEAKNESS. ANAL AND GENITAL LOSS OF FEELING OR NUMBNESS, REFERRED TO AS SADDLE ANAESTHESIA. SUDDEN ONSET OF BLADDER AND/OR BOWEL DISTURBANCE, SUCH AS RETENTION (UNABLE TO PASS URINE) OR INCONTINENCE. SEXUAL FUNCTION MAY ALSO BE DISTURBED. SPINEWORKS
DROP FOOT etc • MEDICAL TREATMENT – FOR ABSCESSES, INFLAMATORY CONDITIONS. • SURGICAL TREATMENT: • TIMING CONSIDERATIONS • DECOMPRESSION • FORAMINAL PROBLEMS • PAINLESS FOOT DROP SPINEWORKS
TRAUMATIC CENTRAL CORD SYNDROME • THORBURN IN 1887. • HYPEREXTENSION WITHOUT # OR DISLOCATION • CAUSES NARROWING BY OVERLAP OF FACETS AND LIGAMENTUM FLAVUM BUCKLING. • 44% OF ALL CLINICAL SYNDROMES AFTER SCI. • MOST FREQUENTLY ENCOUNTERED INCOMPLETE S.C.I. • PRESENT WITH DISPROPORTIONATE WEAKNESS OF UPPER LIMBS, VARIABLE SENSORY LOSS AND BLADDER DSYFUNCTION. • MECHANISM = #, DISLOCATION, PIVD AND FORCED HYPEREXTENSION. • 50% = SPINAL STENOSIS • 50% = RECOVERY • SURGERY FOR SUSTAINED CORD COMPRESSION NOT EMERGENCY SURGERY. SPINEWORKS
ESTABLISHED S.C.I. • NURSING – PRESSURE SORES • BOWELS - ENEMAS ETC • BLADDER- CATHETERISATION • CARDIO-VASCULAR SPINEWORKS
CARDIOVASCULAR EFFECTS OF S.C.I. • REQUIRE PROMPT MEDICAL ATTENTION TO PREVENT NEUROLOGICAL COMPROMISE, MORBIDITY AND DEATH IN ACUTE PHASE – 30 DAYS. • HYPOTENSION, AUTONOMIC CHANGES AND CARDIAC ARRYTHMIAS DUE TO LOSS OF SYMPATHETIC CONTROL WITH LESIONS AT T6 OR HIGHER. • NEED: MONITORING, MEAN BP OF 85, RECOGNITION OF AND TREATMENT OF ANY NEUROGENIC SHOCK OR CARDIAC ARRYTHMIAS AND TREATMENT OF ANY AUTONOMIC CHANGES. • ALSO HIGH RISK FOR DVT; MECHANICAL AND CHEMICAL PROPHYLAXIS. SPINEWORKS
ALL CLEAR NOW SPINEWORKS