Download
1 / 92
920 likes | 1.06k Views
PHLEBOTHROMBOSIS. MUDr. Monika Laššánová. THROMBOSIS. = INTRAVITAL COAGULATION OF BLOOD IN VESSELS OR HEART Incidence of venous thromboembolism – 0,1% 0,01% among people appr . 20 years old 1,0% among people appr . 60 years old.

E N D
PHLEBOTHROMBOSIS MUDr. Monika Laššánová
THROMBOSIS = INTRAVITAL COAGULATION OF BLOOD IN VESSELS OR HEART • Incidenceofvenousthromboembolism– 0,1% • 0,01% amongpeopleappr. 20 yearsold • 1,0% amongpeopleappr. 60 yearsold
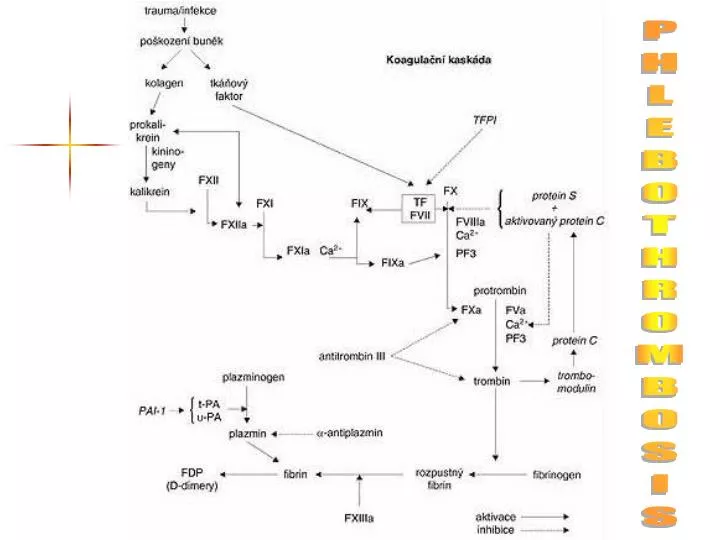
Patogenesisofthrombosis=(1856) – Wirchow´strias activation of COAGULATION = activity of TXA2, activity of anticoagulant sys. (AT III), levels or activation of coagulation f. ... slow BLOOD FLOW = stasis, travelling by airplain, heart failure, paraplegia, immobilisation, pregnancy, varixes, operations, fractures ... deffect of the VESSEL WALL – by damage of endothelium production of PGI2 => proaggregatory activity Most important factors
Arterial thrombi = white • Thrombocytes • Tight adherence => obturation = periferal ischemia • Prevention = antiaggregants • Venal thrombi = red • Fibrinal tail • Weak adherence => risk of embolisation • Prevention = anticoagulants • Recent thrombi • Are removed by thrombolytics = fibrinolytics
Clinicalconditionsincreasingthe risk ofthrombosis arterial: • atherosclerosis • smoking • hypertension • diabetes mellitus • LDL • TAG • + familyhistory • deffectofleft • highdosesofsyntheticoestrogens • polyglobulia … venous: • generalsurgery • orthopedicalsurgery • trauma, malignities, sepsis • immobilisation • congestivefailure • nephrotic syndrome • obesity • varixes • postphlebitic syndrome • oestrogens • pregnancy
Different! thrombophlebitis phlebothrombosis
THROMBOPHLEBITIS • primarily caused by mechanical, microbial or chemical irritation inflammation of vessel wallsecondarily thrombosis – thrombus firmly adhering to vessel wall embolisation only occasionally • clinically:local syndrome = inflammated superficial vein, can be palpated, skin above is red, warm, with significant pain and sensitivity, no big oedema, no general symptoms or only subfebrility • complications: (rarely) early – spreading of inflammation to deep venous sys., late – sec. chronic venous disease = postphlebitic syndrome
DeepVenousThrombosis= Phlebothrombosis + it´s most dangerous complication = pulmonary embolisation (PE) – belong (after IHD and hypertension) among the most common CV diseases in hospitalised patients • PE - 10% of autopsial material • 85% of PE is caused by deep venous thrombosis
PHLEBOTHROMBOSIS (PT) • deepveinsoflowerextremities • primarilyobturationofveinwiththrombus and secondarilyinflammatoryreaction • releasedthrombus = embolus • clinically:oftenasymptomatic – or littlesymptoms = dg. only 30-50% • oedema – asymmetric • pain – spontaneous, compressive – mostlywhilehangingdownthelimb, spasms, feelingofstrain • symptomsofblockedbloodflowfromthelimb (erythema- pale skin- cyanosis) • collaterals –formingafterseveraldaysofobturation ascompensatorymechanism, • systemicsymptoms – notspecific (ifthereis no PE)
Clinicalsymptoms Lowerlimb: • pain • oedema( 1,5 cm) • posit. palp. maneuvers(Homans, Lőwenberg,...) • enlargedsuperficialcollaterals • changeof skin color and temperature
Complicationsof PT • EMBOLUS - released thrombus, carried by the blood flow– mainly to pulmonary artery pulmonary embolisation • Repeated small embolisation (successive) =>chronic pulmonary hypertension => cor pulmonale chronicum • Chronic venous insufficiency
Diagnosisof DVT • + • Kontrastná venografia • Impedančná pletysmogr.
Goalsofthetreatmentof PT • save the patient´s life • avoid occurance of pulmonary embolism • initialise / speed-up resolution of thrombus/embolus • accelerate symptom regression • prevention of recurrency • reduce long term mortality
nonpharmacologic limb elevation (15-20º) earlymobilisationaftersurgery regularexercisewithlegs in bed elastic, specialtights walking pharmacologic lowdosesofheparin(5000 IU) (beforeoperation, duringpostoperationperiodat risk patients), LMWH, fondaparinux Preventionof PT
Antithrombotics Antiaggregatory drugs Anticoagulants Thrombolytics (inh. platelets) (inh. coagulatory factors) (dissolve thrombus)
Antithrombotics • antiaggregants(antiplateletdrugs) = blockFORMATIONofthrombus • anticoagulants= blockGROWTH ofthrombus • thrombolytics(fibrinolytics) = DISSOLUTIONofalreadyformedthrombus
Antiplateletdrugs Anticoagulants Thrombolytics
Anticoagulants • DRUGS ARTIFICIALLY INDUCING “DISTURBANCES“ OF BLOOD COAGULATION • GOAL: TO PREVENT THROMBOSIS OR TO PREVENT FURTHER GROWTH OF THROMBUS
ANTICOAGULANTS DIRECT INDIRECT • Indirectinhibitorsofthrombin and factorXa • Heparin (IIa : Xa) • LMWH (IIa : Xa) • enoxa-, fraxi-, dalte-, revi- • Fondaparinux( Xa) • Directinhibitorsofthrombin • Hirudin, bivalirudin, desirudin • Dabigatran – p.o. = gatrans • DirectinhibitorsoffactorXa • Rivaroxaban – p.o. = xaban • Apixaban– p.o. • Warfarin • Etylbiskumacetate • Phenprocoumon • Dicumarol
Fondaparin Idraparin Rivaroxaban Apixaban indirectanticoag. f. II., VII., IX., X Dabigatran Hirudin, Desirudin indirectinhibitorsofthrombin
HEPARIN • INDIRECT INHIBITOR OF THROMBIN • SUBSTANCE PRESENT ALSO IN OUR BODY (MAST CELLS), USED FROM 1916 • MW = 3 - 30 000 D (15 000 D) • produced from intestinal mucosa of porcine or cattle lungs => quantified in IU • heterogenous mucopolysacharid, anion (´-´ charge) • ACTIVITY IS DEPENDENT FROM THE PRESENCE OF A N T I T H R O M B I N III.
MechanismofActionofHeparin - + 1000x H inactivates already activovated coagulation factors IIa,Xa
Effectsofheparin • Anticoagulatory activity • Weak inhibition of platelet function - adhesivity and aggregation • Weak stimulation of fibrinolysis • releasing of lipoproteinic lipase clearing of lipemic plasma anti - IIa : anti –Xa = 1 : 1
Advantagesofheparin • acts very quickly or immediately, but shortly • has massive effect • it has an antidote -protamine
Disadvantagesofheparin • only injection (i.v., s.c.), • i.m. – no, irregular absorption and haematoma • T1/2 is variable, prolonged with dose, • unpredictable anticoagulant effect – wide variability (for different binding to proteins and unpredictable absorption after s.c. admin.) • possibility of disease reactivation after stopping administration (rebound efect) • control:aPTT (reflects effect to thrombin) – extension to 1,5-2,5 x of norm
Indicationsofheparin • Prophylaxis of vein thrombosis • Th. of deep vein thrombosis and pulmonary embolia • Acute coronary syndroms (Th) • Obturation of peripheral arteries • Hemodialysis, DIC
ADR ofheparin • Bleeding • H. inducedthrombocythopenia(HIT) – lessserious, earlyf.; more seriousf. after5 and days • Allergy • Reversiblealopecia • Possibleosteoporosis in caseoflong-termuse
LOW-MOLECULAR-WEIGHT HEPARINS (LMWH) • INDIRECT INHIBITORS OF THROMBIN • smaller molecules, MR 5 000 D • INHIBIT MORE ANTI-Xa • PRODUCED BY CHEMIC OR ENZYMATIC DEPOLARISATION OF H • ACTIVITY DEPENDS ON THE PRESENCE OF A N T I T H R O M B I N III
Mechanismof LMWH Action anti - IIa : anti -Xa 1 : 2 - 4
Indicationsof LMWH • Preventionofthromboembolia (abdominal and orthopedicsurgery) • Preventionofischemiccomplicationsatacutecoronarysyndroms (unstableanginapectoris, NSTEMI myocardialinfarction) • Therapyofphlebothrombosis and pulmonaryembolism • Hemodialysis
Advantagesof LMWH • Predictableresponse to doseaccordingtoweight • Longerplasmatichalf-life (1-2 s.c. injections per day) • Lower risk ofthrombocytopenia, bleeding and thrombosis • Heparin and LMWH canbeadministeredduringpregnancy and lactation
Fondaparin Idraparin Rivaroxaban Apixaban indirectanticoag. f. II., VII., IX., X Dabigatran Hirudin, Desirudin directinhibitorsofthrombin
FONDAPARINUX • INDIRECT INHIBITOR OF THROMBIN • SYNTHETIC PENTASACHARID SPECIFICALLY INHIBITING FACTOR Xa • MR = 1 700 D • activity depends on the presence of A N T I T H R O M B I N III • doesn´t have the long chain needed for bridging to ATIII. and f. IIa • 300X ability to inactivate f. Xa
AdvantagesofFondaparinux • of bleeding complications • administered s.c. • relatively long lasting effect • highly predictable effect • doesn´t influence aggregation of platelets doesn´t induce thrombocythopenia • disadvantage = price, no antidote
Fondaparin Idraparin Rivaroxaban Apixaban Indirectanticoag. f. II., VII., IX., X Dabigatran Hirudin, Desirudin directinhibitorsofthrombin
HIRUDIN, BIVALIRUDIN • PRIAMY INHIBÍTOR TROMBÍNU • špecificky IREVERZIBILNEINAKTIVUJE TROMBÍNBEZ potreby prítomnosti AT III. • je prirodzený inhibítor zrážania krvi získavaný z pijavíc (hirudo medicinalis) • vyrába sa DNA REKOMBINANTNOU technikou
HIRUDIN, BIVALIRUDIN • DIRECT INHIBITOR OF THROMBIN • SPECIFICALLY IRREVERSIBLYINACTIVATES THROMBINWITHOUT THE NEED FOR AT III • NATURAL INHIBITOR OF BLOOD COAGULATION GAINED FROM LEECH (HIRUDO MEDICINALIS) • PRODUCED BY DNA RECOMBINANT TECHNOLOGY
MA HIRUDINBINDS TO THROMBIN AND irreversibly FORMS AN INACTIVE COMPLEX BIVALIRUDIN-synthetic fragment of hirudin - reversible inhibition of thrombin - duration of action appr. 25 min.