Download
1 / 21
210 likes | 499 Views
Treatment of status asthmaticus. 賴妍如. Reference. REVIEW SERIES: The pulmonary physician in critical care • 12: Acute severe asthma in the intensive care unit Thorax 2003;58:81-88 Clinical review: Severe asthma Critical Care 2002,6:30-44

E N D
Reference • REVIEW SERIES: The pulmonary physician in critical care • 12: Acute severe asthma in the intensive care unit • Thorax 2003;58:81-88 • Clinical review: Severe asthma • Critical Care 2002,6:30-44 • Pathogenesis and management of status asthmaticus in adults (2006 UpToDate ) • Mechanical ventilation in adults with status asthmaticus (2006 UpToDate)
Status asthmaticus • Severe attacks of asthma poorly responsive to adrenergic agents and associated with signs or symptoms of potential respiratory failure
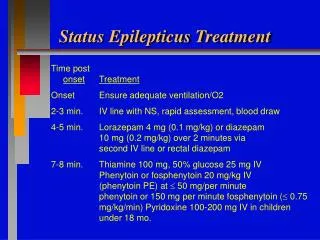
Treatment • Administration of oxygen • β2-agonists (by continuous or repetitive nebulisation) • Systemic corticosteroids • Subcutaneous administration of epinephrine or terbutaline should be considered in patients • not responding adequately to continuous nebulisation, • unable to cooperate, • Intubated patients not responding to inhaled therapy. • Intubated and mechanically ventilated • based mainly on clinical judgment • should not be delayed once it is deemed necessary • should be appropriately sedated • Permissive hypercapnia, increase in expiratory time, and promotion of patient-ventilator synchronism
Inhaled β2-agonists • Continuous or repetitive nebulisation of short-acting β2-agonists • the most effective means of reversing airflow obstruction • More effective and induces less hypokalaemia when delivered by the inhaled route • Salbutamol (albuterol) is the most frequently used agent because of its potency, duration of action (four to six hours) and β2-selectivity • 2.5 mg (0.5 ml) in 2.5 ml normal saline by nebulisation continuously or every 15–20 min until a significant clinical response is achieved or serious side effects appear • Intravenous administration should be considered in patients who have not responded to inhaled or subcutaneous treatment, in whom respiratory arrest is imminent
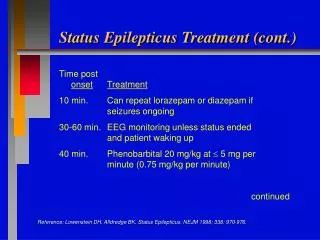
Corticosteroids • Should begin much earlier, at the first sign of loss of asthma control • Early treatment with adequate doses of corticosteroid improves outcome • Reduce mortality • Controversy about the optimal dose of corticosteroid • No particular advantage of the intravenous over the oral route provided there is reliable gastrointestinal absorption
Ipratropium • Ipratropium bromide has a mild additional bronchodilating effectwhen added to ß agonists that may only be significant in severe asthma • Ipratropium bromide 0.5 mg by nebulisation every 1–4 hours, combined with salbutamol
Aminophylline • The addition of aminophylline does notadd to the bronchodilating effect of optimal doses of ß agonists • Not recommended as a first line drug in acute asthma management • Its inclusion as a second line agent is still debated
Subcutaneous epinephrine and terbutaline • Should be considered in patients • not responding adequately to continuous nebulised salbutamol • unable to cooperate • intubated patients not responding to inhaled therapy • 0.3–0.4 ml of a 1:1000 solution subcutaneously every 20 min for 3 doses
Mechanical ventilation • Cardiopulmonary arrest and deteriorating consciousness are absolute indications for intubation and assisted ventilation • Hypercapnia, acidosis, and clinical signs of severe disease at presentation may not require immediate intubation before an aggressive trial of conventional bronchodilator therapy • Conversely, progressive deterioration with increasing distress or physical exhaustion may warrant intubation and mechanical ventilation without the presence of hypercapnia
Mechanical ventilation • Correction of the hypoxemia is one of the first priorities • To avoid further significant increase of lung hyperinflation • Decrease of VE • Increase of expiratory time • Decrease of resistance • Controlled hypoventilation (Permissive hypercapnia (PaCO2 does not exceed 90 mmHg) with an associated acidosis (pH 7.2–7.15)) • Decreasing either the tidal volume or the respiratory frequency, or both • The recommended strategy to reduce lung hyperinflation • Pressure-controlled ventilation seems more appropriate to maintain airway pressure especially in status asthmaticus
Mechanical ventilationNeuromuscular-blocking agents • Lessens the patient -ventilator asynchronism • Lowers the risk for barotrauma • Reduce oxygen consumption and dioxide production, and reduces lactate accumulation • Disadvantages: myopathy, excessive airways secretions, histamine release (atracurium), and tachycardia and hypotension (pancuronium). • Currently the use of paralytics is usually recommended only in those patients who cannot adequately be controlled with sedation alone
THERAPEUTIC OPTIONS IN THE NON-RESPONDING PATIENT • Manual compression • Mucolytics • Inhalational anaesthetic agents • Helium • Magnesium sulphate • Leukotriene inhibitors • Platelet activating factor (PAF) inhibitors • Nitric oxide (NO)
Manual compression • Hyperinflation is relieved by manual compression of the chest wall during expiration • Has not been fully evaluated by a controlled clinical study in humans
Mucolytics • Chest physiotherapy and mucolytics have no proven benefit • Bronchoscopic lavage with locally applied acetylcysteine may be used to help clear impacted secretions in selected refractory patients but its routine use is not advocated
Inhalational anaesthetic agents • Halothane, isoflurane, and sevoflurane are potent bronchodilators in asthmatic patients receiving mechanical ventilation who have failed to respond to conventional ß adrenergic agents • Sevoflurane, a halogenated ether, is largely devoid of cardiorespiratory side effects and may be the preferred agent
Helium • A mixture of helium and oxygen (heliox) may reduce the work of breathing and improve gas exchange because of its low density that reduces airway resistance and hyperinflation • However, the benefits are marginal and the concentration of inspired oxygen is consequently decreased • The use of heliox to prevent intubation has not been studied • But dyspnoea scores were improved in one study, possibly by reducing the work of breathing
Magnesium sulphate • Early anecdotal reports suggested benefit from intravenous magnesium sulphate, which has been inconsistently supported by randomised studies • A significant benefit was recently observed in children receiving intravenous magnesium sulphate (40 mg/kg) during acute asthma attacks
Leukotriene inhibitors • relatively minor role • Platelet activating factor (PAF) inhibitors • attenuate the late response in asthma but have limited clinical efficacy • Nitric oxide (NO): • weak bronchodilator effect. • It dilates pulmonary arteries • When inhaled, may improve ventilation/perfusion matching