Download
1 / 16
160 likes | 291 Views
Modeling & Simulation What can they offer?. March 28, 2012 Ottawa, ON Waiting Time Management Strategies for Scheduled Health Care Services: A Workshop for Researchers, Managers and Decision-makers. The Operations Research Toolkit. Patients. People. Resources.

E N D
Modeling & Simulation What can they offer? March 28, 2012 Ottawa, ON Waiting Time Management Strategies for Scheduled Health Care Services: A Workshop for Researchers, Managers and Decision-makers
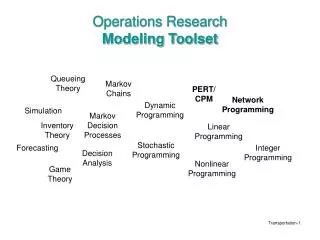
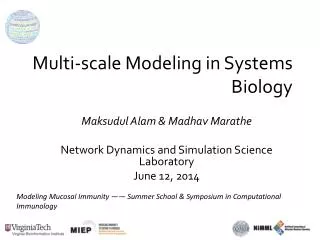
The Operations Research Toolkit Patients People Resources Long Range Demand Forecasting Long Range Supply Forecasting Capacity Planning & Allocation Strategic Patient Scheduling Models HHR Scheduling Resource Scheduling Tactical Managing Demand Variability Managing Supply Variability Analysis of Pathways Operational
Urgent Patient Queueing Model • Objective: To develop a generalized model to determine how to best allocate capacity to urgent patients • Scope: Any fixed capacity intervention with 2 urgency classes and a critical MAWT to meet for the high urgency class (Winnipeg, Edmonton) • Modelling methodology: Stochastic Model to create closed-form Queueing formulas, tested against DES (Arena) models
Rationale • Goal: Provide more certainty around surgery dates for all patient classes • Patient Scheduling variability depends upon: • OR Schedule stability • Cancellations of OR time, frequency of scramble time • Surgeon variability • Longer waitlists create more uncertainty of surgeon availability • Patient readiness • Prehab and case management has improved this • Arrival of urgent patients that ‘bump’ elective patients when there isn’t adequate time reserved
Literature Overview • Scheduling Policies for managing Urgent/Elective • Patrick & Puterman (2008) “Dynamic Multipriority Patient Scheduling for a Diagnostic Resource • CT Scans for 3 outpatient categories, MAWT of 7, 14, 28 days • Markov Decision Process (MDP) that recommends that highest priority gets scheduled right away and that lower priorities are scheduled into the latest appointment available to meet MAWT. When demand > capacity, higher priority patients are rejected vs. a bumping of elective. • Increased flexibility with high priority scheduling improves system • Zonderland et al. (2010) “Planning and scheduling of semi-urgent surgeries. • Stochastic model created for specific location. • Difficult to multi-location replicate due to mathematical approach
Research Question • What is the ‘optimal’ number of urgent surgical slots to set aside so as to meet a desired performance metric – specifically % of urgent patients that bump electives • Required data: • Patient arrival rate • MAWT for urgent patients • Output: • Minimum # of surgeries to reserve of MAWT window
Simulation Approach Average arrival rate of urgent patients = 1 per week. Surgery rate = Number of urgent surgical spots reserved over the next 4 weeks for urgent patients
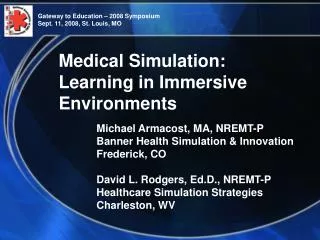
a5+ a4 a3 a2 a2 a2 a2 a2+ a1 a1 a1+ = 1-a0 a1 0 1 2 3 4 5 a1 a1 a0 a0 a0 a0 a0 a0 a5+ a4 a4+ a3 a3 a3+ Stochastic Model Approach • ‘Simple’ representation of urgent patient arrival process • Ability to calculate, with relative ease & accuracy, the effect of reserving capacity for urgent patients A stochastic model may be used rather than a simulation
Analytical Queueing Model • Derive appropriate formulae based upon an M/D/1/N queueing model • Test accuracy of queuing model against DES • Implement formula in Excel front-end The stochastic model may be solved analytically to determine the probability of having 0, 1, …N patients waiting.
Next Steps • Phase I - Data gathering and Implementation of logic into Concordia Scheduling Software, early 2012 • Phase II - Integrate into Generalized DES Model as part of “best practices” options • Phase III - Improve user interface and test at pilot clinics – gather performance feedback