Download
1 / 30
310 likes | 667 Views
Melanoma – Natural History and Principles of Treatment. Melanoma Patient Symposium YNHH – Smilow Cancer Hospital Sept 11, 2014. What is Melanoma?. Cancer of cells which are responsible for all types of body pigmentation (melanocytes)

E N D
Melanoma – Natural History and Principles of Treatment Melanoma Patient Symposium YNHH – Smilow Cancer Hospital Sept 11, 2014
What is Melanoma? • Cancer of cells which are responsible for all types of body pigmentation (melanocytes) • Melanocytes are primarily present in skin but are also present in the eye and mucous membranes (head sinuses, oral cavity, rectum/anus, vulva/vagina) • Some types of melanoma are related to sun exposure and sunburns • Malignant cells gain special properties through genetic (mutations) and other cell changes • Uncontrolled growth • Ability to travel in blood and lymphatics to other organs • Can implant in other organs and divide and grow (metastases) • Can remain dormant for years before growth is triggered • Dormant state cannot be detected by scans or other tests
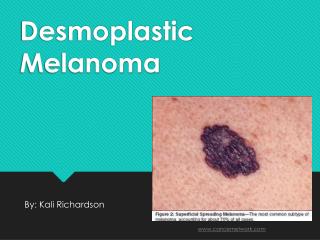
A - asymmetry B – borders irregular C – color variation D - diameter E- evolution F – funny looking
Skin Ocular Nasal Vulvar Anorectal Acral-lentiginous
Primary Tumor Skin Mucosa Ocular Biology of Dormancy Not Understood Local (Lymphatic) Dissemination Local recurrence In-transit metastases Regional node involvement Hematogenous Dissemination Skin Lung Lymph node Liver Bone GI/mesentery CNS (+ leptomeninges) ? years
25-30% at presentation of systemic mets, 60-70% of all patients subsequently
Treatment of Primary Melanoma • Excisional biopsy by dermatologist • Greater than 90% present without distant metastases • Referral to surgeon • Wide local excision – margins ≥ 2cm for lesions > 1mm thick • Sentinel Node Biopsy in regional basin • For lesions > 0.75 thick • For prognostic information – does not affect outcome • In very high risk patients, CT scans or PET scans to rule out distant metastases • Completionlymph node dissection (for positive SLNB)
The Three Important Questions After Complete Resection of Primary Melanoma (and Regional Nodes) • What is my risk that distant metastases will be found in the future? • What can be done to lower the risk that my cancer might recur? • How will I be monitored to detect the cancer if it recurs?
Staging is Used to Provide Risk for Distant Recurrence (Distant Metastases) • Risk Factors • Depth of primary • Ulceration under the microscope • Presence of cancer cells in the regional nodes (from the sentinel node biopsy and complete lymph node dissection)
Principles of Monitoring for Recurrence • No (good) data to understand the impact of frequency of type of monitoring on outcome • Both determined by risk • Views on monitoring may change as more effective therapies are introduced for advanced disease • Evaluation by oncologist every 3 months to 1 year • History, exam, blood work (CBC, liver function, LDH) • CT scans and/or PET-CT scans in high risk individuals every 6 to 12 months • Usually stop monitoring at 5-7 years • Dermatology evaluation 2-4x yearly for detection of second primaries (10% risk)
Options to Reduce Recurrence Risk • Observation • Interferon-alfa • Different dose and schedules • Administration for up to one year • Increases time to recurrence • Reduces overall risk of recurrence by about 10% • Can induce moderate to severe toxicity in some (fever, chills, fatigue, loss of appetite, depression, difficulty in concentration) • Possible new options • Ipilimumab (Yervoy) – not yet approved, data so far similar to interferon, potential for severe toxicity • Clinical Trials – compare potential better agents to standard of care
Management of Advanced Disease • Treat both the lesions seen on scans and areas of disease that have not yet appeared on scans • Surgery, local injection, or radiation not sufficient to eliminate the disease • Requires systemic (intravenous or oral) medications • Use systemic therapies first that can induce long term remissions • Control pain and manage lesions early that may cause early morbidity (pain, bleeding, limitation of function, unacceptable cosmetic appearance) • Screen the brain at baseline and every 8-12 weeks • CT scans of chest/abd/pelvis or CT chest + MRI abdomen/pelvis to ‘stage’ disease • Repeat scans every 6-12 weeks (depends of treatment)
Options for systemic therapies • Clinical Trials • Immune therapies (can give long term remissions) • High dose interleukin-2 (Proleukin) • Ipilimumab (anti-CTLA-4) (Yervoy) • Pembrolizumab (anti-PD-1) (Keytruda) • Nivolumab(anti-PD-1) (Optiva) – approval pending • Targeted therapies (rapid response in most but few have long term control) • BRAF mutation– dabrafenib(dafinlar)/trametinib (mekinist), vemurafenib (zelboraf) • NRAS mutation – investigation MEK + CDK4 inhibitors • C-kit (mucosal and acral-lentiginous melanomas) – imatinib, dasatinib, sorafenib, others • Cytotoxic Chemotherapy (can work rapidly but only in a few and rarely achieve long term control) • Temozolomide (temodar) or dacarbazine • Carboplatin and paclitaxel • Biochemotherapy
Chemotherapy Biochemotherapy 2014 – Treatment Options for Metastatic Melanoma Targeted therapies Immune therapies mBRAF mNRAS mCKIT Interleukin-2 Vemurafenib CDK4i + MEKi cKITi Ipilimumab (anti-CTLA4) Dabrafenib Anti-PD1 (nivolumab) (pembrolizumab) Trametinib (MEKi) Nivolumab + ipilimumab Dabrafenib + Trametinib Vemurafenib + cometinib
no GKS/SRS Brain mets Eligible for Immunotherapy yes C-kit mutation Ckit inhibitor No Mutation analyses Yes CDK4i + MEKi NRAS mutation PD NO mutation BRAF mutation Anti-PD1 Anti-CTLA-4 High dose IL-2 Adoptive Immunotherapy Other Investigational Immunotherapy Trials Yes Phase 1 Other targeted Rx Anti-angiogenesis Supportive care Chemotherapy BRAFi + MEKi BRAFi + other ERKi Yale Cancer Center Melanoma Treatment Algorithm
Il-2 Induced Regression of Melanoma Liver Metastases 6-24-05 11-23-05 Persistent/progressing disease in spleen, SQ buttock, and lung removed; NED x 7 years
Response to Ipilimumab 10 mg/kg x 2 doses 2 baseline brain mets regressed also: No disease progression 5+ years
Metastatic Melanoma, Anti-PD1 1 mg/kg every other week
Overall Survival for Concurrent Therapy by Dose Cohort 100 90 2 Yr OS 88% 1 Yr OS 94% 80 70 60 1 Yr OS 85% 2 Yr OS 79% 50 40 Survival (%) 30 1 Yr OS 57% 2 Yr OS 50% 20 10 Censored 0 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 Nivo 0.3 mg/kg + IPI 3 mg/kg (n=14) Nivo 1 mg/kg + IPI 3 mg/kg (n=17) Nivo 3 mg/kg + IPI 1 mg/kg (n=16) Nivo 3 mg/kg + IPI 3 mg/kg (n=6) Concurrent Cohorts 1-3 (n=53) 14 17 16 6 53 13 17 16 6 52 11 16 15 6 48 10 15 15 6 46 8 15 15 6 44 7 14 13 6 40 7 14 4 6 31 7 13 2 6 28 7 9 0 3 19 7 4 0 0 11 5 3 0 0 8 2 3 0 0 5 2 3 0 0 5 2 2 0 0 4 1 0 0 0 1 1 0 0 0 1 0 0 0 0 0 Pts at Risk Nivo 0.3_IPI 3 Nivo 1 _IPI 3 Nivo 3_IPI 1 Nivo 3_IPI 3 Concurrent Months Presented by: