Download
1 / 48
480 likes | 612 Views
Cancer genetics and treatment BME1450 David Hogg. RJ 47 year male. Presented to family doctor Dec 2003 with pigmented lesion on scalp Told lesion of no significance. Melanoma Types. Superficial spreading melanoma. Nodular melanoma. Lentigo maligna melanoma. Acral lentiginous melanoma.

E N D
RJ 47 year male • Presented to family doctor Dec 2003 with pigmented lesion on scalp • Told lesion of no significance
Melanoma Types Superficial spreading melanoma Nodular melanoma Lentigo maligna melanoma Acral lentiginous melanoma
RJ 47 year male • Lesion began to bleed two months late • Biopsy showed nodular melanoma • Referred to Princess Margaret Hospital melanoma clinic for opinion March 2004
RJ 47 year male • Sent for wide local excision of melanoma • Sentinel node biopsy revealed melanoma in 2/6 regional lymph nodes • Radical neck dissection April 2004: no positive nodes
RJ 47 year male • Treated with Interferon- • While on treatment, developed severe headaches in July 2004
RJ 47 year male • Treated with radiotherapy to brain plus Temozolomide • Died of disease August 2004
The art of medicine lies in amusing the patient while the disease runs its course. Sir William Osler
Cancer – questions and problems • What is Cancer? • What causes the disease? • Why is cancer so difficult to treat? • Where are we going?
Cancer – questions and problems • What is Cancer? • What causes the disease? • Why is cancer so difficult to treat? • Where are we going?
Normal cells - characteristics • Proliferate only when they receive positive growth signals from the environment • Cease growing or die in the absence of such signals • Cease growing or die when they receive growth-inhibitory or death signals
Normal – characteristics: cont… • Differentiate or enter senescence (old age) during their lifetime. • Respect local anatomic boundaries – will not cross tissue barriers unless specifically told to do so. • Do not spread to other areas of the body (metastasize).
Programs/responses Growth factor Growth + No growth + Growth Factor receptor - DNA (genes) Signal transduction pathways Death Inputs Differentiation Tumor suppressor Metastasis Inhibitory factor Genetic targets
Cancer is a genetic disease I • Cancer cells are derived from normal cells • To progress from a normal cell to a malignant one, a series of changes in the DNA of the cell must occur • These changes alter the behaviour of the cell.
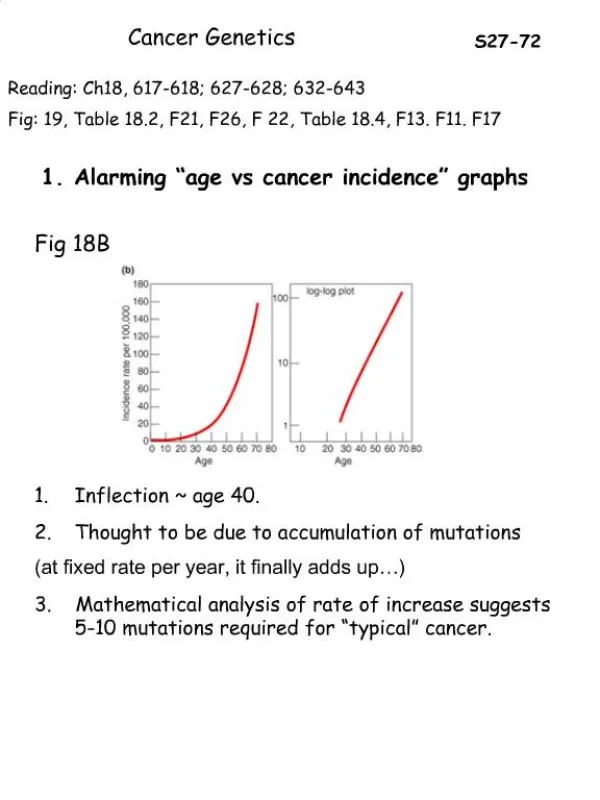
Cancer is a genetic disease II • In almost all cases, a cell must suffer multiple genetic ‘hits’ to become fully malignant. • The number of hits is thought to number about 5-7 in most types of cancer • In many cases, at least some of these genetic lesions are known, and may differ between different types of cells (and hence cancer types).
Tumor progression – sequential mutations s1 s2 s3 s4
Timing of genetic changes • There is not always a set pattern of genetic changes as a cell progresses to malignancy. • In other words, although 5-7 changes must occur to make a cell fully malignant, the order and timing of these alteration may be flexible.
Implications of progressive genetic alterations • Cancers are not cells with “uncontrolled growth”! • Loss of growth control occurs very slowly over several years, in a stepwise fashion. • Therefore, defining the genetic changes in a tumor will become as important as histological study.
Melanoma Types Superficial spreading melanoma Nodular melanoma Lentigo maligna melanoma Acral lentiginous melanoma
Normal Skin Benign Nevus Dysplastic Nevus (DN) Melanoma: a multistage process Radial Growth Phase melanoma Vertical Growth Phase melanoma Derived in part from Chin et al. (1998) Genes Dev. 12: 3467-3481
SMAD4DCC APC (FAP) K-ras p53 MMR (HNPCC) Adenocarcinoma c-src/Cox2 Normal colon DN gene?(DNS) CDKN2A(Familial melanoma) p53 Normal melanocyte Invasive melanoma Ras? - 10q - 6p Timing of genetic lesions in melanoma
Cancer – questions and problems • What is Cancer? • What causes the disease? • Why is cancer so difficult to treat? • Where are we going?
What causes genetic changes? • Environment • Radiation, drugs (eg: chemotherapy); infections; etc • Genetic background • Inherited (germline) mutations • Tendency to develop genetic lesions (DNA repair deficiencies).
Tumour Formation Genotype Somatic Mutations Environment
But remember throughout that no external cause is efficient without a predisposition of the body itself. Otherwise, external causes which affect one would affect all... Galen, 200 A.D.
Familial Cancer • Now known to occur in many tumor types egs: • Breast (BRCA1; BRCA2) • Colon (APC; MLH1; MSH2; PMS1; PMS2) • Melanoma (CDKN2A) • Retinoblastoma (RB) • Li-Fraumeni Syndrome (p53)
Familial Cancer - Characteristics Compared to the corresponding sporadic cancers: 1. Age at first presentation is lower 2. Tumors may present at multiple sites in the same tissue 3. Tumors may occur in different tissues 4. There may be a family history
Melanoma family - example I:1 I:2 melanoma II:1 II:2 II:3 II:4 II:5 II:6 II:7 multiple melanoma brain melanoma melanoma myeloma Dx33 2 primaries
Loss of a functional tumor suppressor gene g s A2* A1 A2 A1 A2* Loss of remaining normal allele Normal Mutation of one allele
LOH of the wild-type CDKN2A allele in sorted BM obtained from multiple myeloma patient I:1 I:2 melanoma II:1 II:2 II:3 II:4 II:5 II:6 II:7 multiple melanoma brain melanoma melanoma myeloma Dx33 2 primaries Heteroduplex Mutant Wild-type Unsorted BM Germline DNA Sorted BM (myeloma)
Knudson’s Two-Hit Model Mendelian Sporadic Germlinemutation Normal gene Somatic mutation Somatic mutation Somatic mutation Multiple Tumors Bilateral Early-onset Single Tumors Unilateral Later-onset
Familial Cancer - Characteristics Compared to the corresponding sporadic cancers: 1. Age at first presentation is lower 2. Tumors may present at multiple sites in the same tissue 3. Tumors may occur in different tissues 4. There may be a family history
Familial Melanoma • ~ 10% of melanoma patients have at least one affected family member • Only ~3% of patients have multiple affected relatives • However, the risk for patients with a predisposition to melanoma is very high: ~60-80X that of the general (European) population
Germline mutations in the CDKN2A gene that predispose to melanoma - Toronto families 24ins 19del insertion 14del 6del 2del E3 deletion E2 CDKN2A E1 3’ UTR 5’ I49S T93P S56I missense V57I A5T D85T G122V R24P M53I G-34T V126D
Problems in Treating Cancer If a cancer depends on at least 5-7 mutations in different pathways, and these pathways differ from cell to cell, then how: 1. Do we identify critical pathways in the cell 2. Determine the critical components of each pathway?
“The most effective way of destroying a network is to attack its most connected nodes” Yuhai Tu, Nature 2000
Tools • For testing pathways: • Cell lines • Tumor biopsies from patients • To knock out specific mRNA: • siRNA • To affect specific proteins: • Drugs • Delivery/attack: ?viruses
Melanoma treatment with an oncolytic virus, JX-594 (Mastrangelo et al., Cancer Gene Therapy, 6: 409, 1999)