Download
1 / 33
390 likes | 906 Views
CPAP. Continuous Positive Airway Pressure. Objectives. Define CPAP Understand pathophysiology EMS applications Protocol implementation. What is CPAP???.

E N D
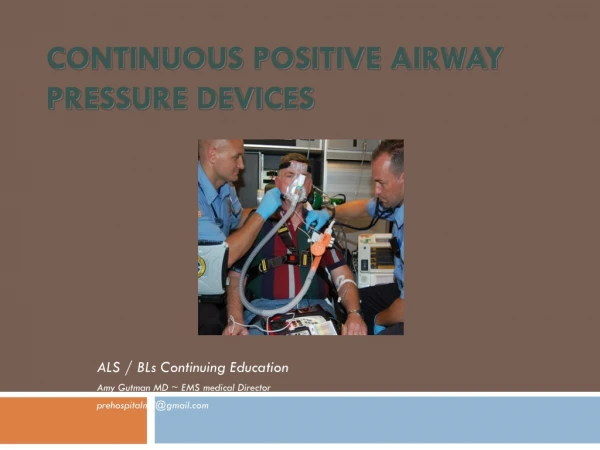
CPAP Continuous Positive Airway Pressure
Objectives • Define CPAP • Understand pathophysiology • EMS applications • Protocol implementation
What is CPAP??? • CPAP increases pressure in the lungs and holds open collapsed alveoli, pushes more oxygen across the alveolar membrane, and forces interstitial fluid back into the pulmonary vasculature. • This improves oxygenation, ventilation and ease of breathing. • The increased intrathoracic pressure decreases venous return to the heart and reduces the overwhelming preload (pressure in the ventricles at the end of diastole). • This lowers the pressure that the heart must pump against (afterload), both of which improve left ventricular function.
Pressure Gradient So why does oxygen pass into the blood? Deoxygenated blood has a lower partial pressure of oxygen than alveolar air so oxygen transfers from the air into the blood.
7.5cm H20 CPAP CPAP alters the pressure gradient! 1cm H2O is equal to 0.735mm Hg. 7.5cm H2O CPAP increases the partial pressure of the alveolar air by approximately 1%. This increase in partial pressure ‘forces’ more oxygen into the blood. Even this comparatively small change is enough to make a clinical difference.
Perfusion • Refers to the process of circulating blood through the pulmonary capillary bed • In order for perfusion to occur, the following must be intact: • A properly functioning heart (pump) • Proper vascular “size” • Adequate blood volume / hemoglobin
The Requirements Of CPAP • The real requirement is for Continuous CONSTANT Positive Airway Pressure • A stable airway pressure as prescribed in order to reduce work of breathing (WOB)
CPAP is oxygen therapy in its most efficient form. • Simple Masks • Venturi Masks • Humidifiers • CPAP
Important Aim Of CPAP Is To Increase Functional Residual Capacity (FRC) • Volume of gas remaining in lungs at end-expiration • CPAP distends alveoli preventing collapse on expiration • Greater surface area improves gas exchange
Physiological Effects Of CPAP • Increases PSO2 • Increases FRC • Reduces work of breathing
Indications for Use • Treatment of severe respiratory distress CHF/COPD/Asthma • RR>25 bpm • Retractions, accessory muscle use or fatigue • SAO2 < 94% at any time • Near drowning • Pt must be able to maintain own airway and be able to follow commands.
Exclusion Criteria • BP <90 mmHg • Unconscious • Inadequate respiratory rate • Cardiac arrest • Unable to obtain adequate seal • Pnuemothorax • Active emesis
CPAP And Pulmonary Edema • Severe pulmonary edema is a frequent cause of respiratory failure • CPAP increases functional residual capacity • CPAP increases transpulmonary pressure • CPAP improves lung compliance • CPAP improves arterial blood oxygenation • CPAP redistributes extravascular lung water (Rasanen 1985)
Benefits/Advantages of CPAP • CPAP reduces work of breathing by keeping the “wet” alveoli open • If the alveoli are open at the end of expiration, energy is not consumed on the next inhalation • Work of breathing is reduced relieving respiratory muscle fatigue
Benefits/Advantages of CPAP • A higher alveoli pressure will result in a stoppage of fluid movement into the alveoli • Increase in airway pressure results in improved gas exchange
CPAP And Acute Respiratory Failure • CPAP overcomes inspiratory work imposed by auto-peep • CPAP prevents airway collapse during exhalation • CPAP improves arterial blood gas values • CPAP may avoid intubation and mechanical ventilation (Miro 1993)
Important Point • Emphysema patients do not respond predictably to CPAP
As a general rule… • The larger the “barrel chest” and the more pronounced the accessory muscles, the more caution we should use with CPAP
What is needed for CPAP application. • Oxygen source capable of producing 50 psi. • Flow regulator which delivers either a fixed oxygen concentration at 30% or an adjustable flow regulator. • Venturi • Micro channels • Tight fitting mask to which the oxygen/air mixture output of the generator is attached and applied to the patient. • Positive End-Expiratory Pressure (PEEP) valve connected to the exhalation port which maintains a constant pressure in the circuit. • What are some signs and symptoms of respiratory distress??
What is needed for CPAP application. • Oxygen source capable of producing 50 psi. • Flow regulator which delivers either a fixed oxygen concentration at 30% or an adjustable flow regulator. • Venturi • Micro channels • Tight fitting mask to which the oxygen/air mixture output of the generator is attached and applied to the patient. • Positive End-Expiratory Pressure (PEEP) valve connected to the exhalation port which maintains a constant pressure in the circuit. • What are some signs and symptoms of respiratory distress??
CPAPContraindications • CPAP may be contraindicated for patients with any of these conditions: • Unconscious • Apnea • Pneumothorax • Decreased cardiac output and gastric distention • Severe facial injury • Hypotension secondary to hypovolemia • Uncontrolled vomiting
Explain the Procedure to your Patient • Explain to your patient that in order to get the best possible results from a CPAP device. Ask them to inhale through the nose and exhale through the mouth against the pressure produced by the CPAP machine. • If they do not know what to expect, it is similar to the air felt when sticking your head out of the car window when moving.
The Whisperflow • Here is a step by step review of the operation of the Whisperflow CPAP device. • Properly assess pt for baseline Pulse Oximetry • Attach high pressure hose to portable tankusing short adapter hose. It may be best to load the patient first and start CPAP early in the transport: conserves portable tank for ER transfer. • Assemble mask and tubing, don't forget to place thefilter on air intake of the CPAP device
The Whisperflow Explain the procedure to the patient. Turn the unit on (all the way) & turn the FLOW on (all the way) Prepare mask, strap rearrangement might be necessary Have the patient place the mask on his/her face tightly. Some "coaching" will help the patient transition from holding the mask near their face to creating a seal. It's OK for the patient to hold the mask without using the straps if they're more comfortable that way. When he is comfortable with the feeling of the mask you may secure it to his head tightly so that no leaks are noticed.
Final Application Steps After loading the patient to the unit you'll need to transfer to the onboard oxygen.Do it quickly - turn on the main first! Next you'll need to fine-tune the unit by decreasing the FLOW until a slight outward flow is felt while the patient inhales. You can easily add nebulized albuterol to the patient's treatment by cutting the tubing at a joint and inserting a 'T' and nebulizer with 6 liters oxygen attached. By using the patient's pulse-ox level as a guide you may adjust the amount of oxygen up to achieve desired oxygen saturation, usually 90 -93%.
A few things to remember... • When the flow valve is open all the way, with the oxygen valve closed, you are giving the patient 28% oxygen and a portable tank will last quite some time! • By increasing the oxygen flow, you'll use more liters per minute - as much as 140! Be careful, you'll run out! • If you reach the point that air is blowing out of the air intake on the device your oxygen flow is too high. • When swapping from portable to main oxygen tanks warn the patient that the flow will stop for a few seconds but they will still be able to breathe, then swap quickly!
Oxygen Tanks At 28-30% FiO2 , a full tank should last approximately: • D cylinder=28 minutes • E cylinder=40-50 minutes • M cylinder=about 4 hours • FiO2 is fraction of inspired oxygen. (at 100% FiO2 a D cylinder tank will last approximately 3-4 minutes. Use what you need, but be prepared with additional cylinders)
Case Study for CPAP You are called to a 76-year old male who is complaining of dyspnea. Upon arrival, you find the patient sitting on a chair leaning forward. He is diaphoretic, cyanotic and has a respiratory rate of 48. Upon auscultation you hear fine crackles throughout both lung fields and he is hypertensive. http://www.eresp.com/CPAPosSim.swf
Works Cited and Thank You Thank you to EMS Personnel at Dallas Ambulance, ST Paul Fire, Salem Fire, Rural Metro, Washington Co EMS, MTCI, Albany Fire, Marion County, and Mercy Flights for sharing information regarding CPAP. The following websites were also use as resources. • http://www.dhfs.state.wi.us/ems/EMSsection/Protocols/CPAP/CPAP_Protocol.pdf • http://www.ems1.com/columnists/dan-white/articles/390898-A-Look-at-CPAP-for-EMS • http://caradyne.respironics.com/whisperflow.htm • http://phillydan.spaces.live.com/Blog/cns!B2AD15EED4F62B2B!236.entry • http://elearning.respironics.com/main_ProdTrainCourse_pr.asp • http://www.jcems.net/cgi-bin/news.cgi • http://www.eresp.com/CPAPosSim.swf • http://www.miamitwp.org/fireems/training/skill_sheet_ems.htm • http://www.emsresponder.com/features/article.jsp?id=1738&siteSection=16 • http://www.maconnc.org/ems/CPAP.html • http://www.merginet.com/index.cfm?pg=airway&fn=CPAPuser • http://emsstaff.buncombecounty.org/inhousetraining/cpap/cpap_overview2.htm • http://www.doctorfowler.com/lecturepage.shtml