Download
1 / 1
10 likes | 164 Views
Figure 2. Macro with covariate guided initial dose and Bayesian adaptation to achieve the target concentration (12-15 ng/ml). Population Pharmacokinetics of Tacrolimus in Paediatric Haematopoietic Stem Cell Transplantation and Implementation in a Dose Adaptation Tool

E N D
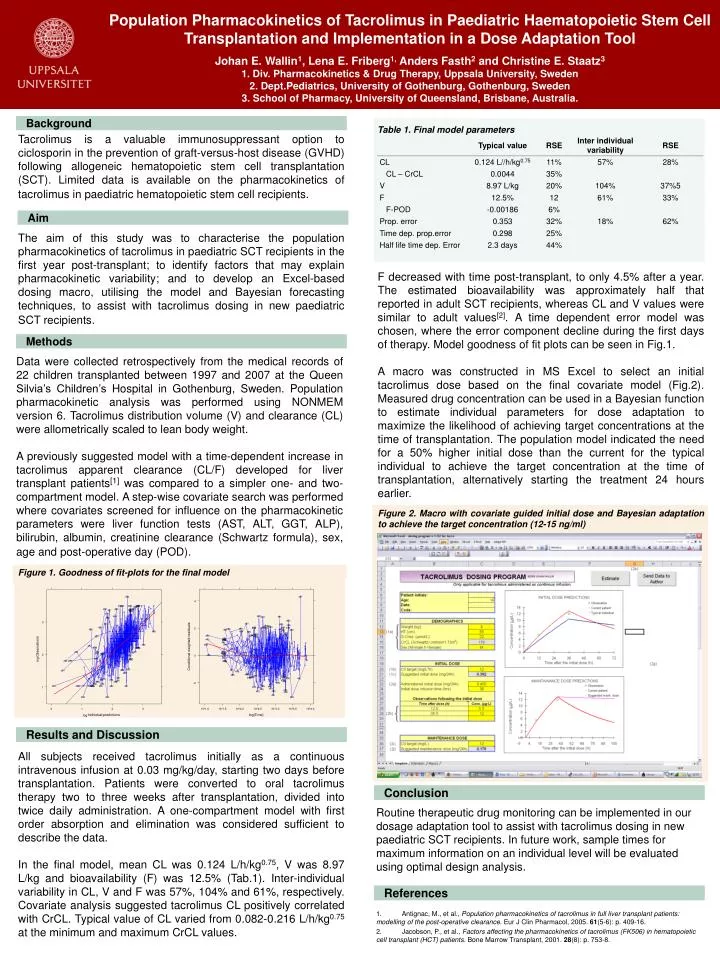
Figure 2. Macro with covariate guided initial dose and Bayesian adaptation to achieve the target concentration (12-15 ng/ml) Population Pharmacokinetics of Tacrolimus in Paediatric Haematopoietic Stem Cell Transplantation and Implementation in a Dose Adaptation Tool Johan E. Wallin1, Lena E. Friberg1, Anders Fasth2 and Christine E. Staatz31. Div. Pharmacokinetics & Drug Therapy, Uppsala University, Sweden 2. Dept.Pediatrics, University of Gothenburg, Gothenburg, Sweden 3. School of Pharmacy, University of Queensland, Brisbane, Australia. Background Table 1. Final model parameters Tacrolimus is a valuable immunosuppressant option to ciclosporin in the prevention of graft-versus-host disease (GVHD) following allogeneic hematopoietic stem cell transplantation (SCT). Limited data is available on the pharmacokinetics of tacrolimus in paediatric hematopoietic stem cell recipients. Aim The aim of this study was to characterise the population pharmacokinetics of tacrolimus in paediatric SCT recipients in the first year post-transplant; to identify factors that may explain pharmacokinetic variability; and to develop an Excel-based dosing macro, utilising the model and Bayesian forecasting techniques, to assist with tacrolimus dosing in new paediatric SCT recipients. F decreased with time post-transplant, to only 4.5% after a year. The estimated bioavailability was approximately half that reported in adult SCT recipients, whereas CL and V values were similar to adult values[2]. A time dependent error model was chosen, where the error component decline during the first days of therapy. Model goodness of fit plots can be seen in Fig.1. A macro was constructed in MS Excel to select an initial tacrolimus dose based on the final covariate model (Fig.2). Measured drug concentration can be used in a Bayesian function to estimate individual parameters for dose adaptation to maximize the likelihood of achieving target concentrations at the time of transplantation. The population model indicated the need for a 50% higher initial dose than the current for the typical individual to achieve the target concentration at the time of transplantation, alternatively starting the treatment 24 hours earlier. Methods Data were collected retrospectively from the medical records of 22 children transplanted between 1997 and 2007 at the Queen Silvia’s Children’s Hospital in Gothenburg, Sweden. Population pharmacokinetic analysis was performed using NONMEM version 6. Tacrolimus distribution volume (V) and clearance (CL) were allometrically scaled to lean body weight. A previously suggested model with a time-dependent increase in tacrolimus apparent clearance (CL/F) developed for liver transplant patients[1] was compared to a simpler one- and two-compartment model. A step-wise covariate search was performed where covariates screened for influence on the pharmacokinetic parameters were liver function tests (AST, ALT, GGT, ALP), bilirubin, albumin, creatinine clearance (Schwartz formula), sex, age and post-operative day (POD). Figure 1. Goodness of fit-plots for the final model log log Results and Discussion All subjects received tacrolimus initially as a continuous intravenous infusion at 0.03 mg/kg/day, starting two days before transplantation. Patients were converted to oral tacrolimus therapy two to three weeks after transplantation, divided into twice daily administration. A one-compartment model with first order absorption and elimination was considered sufficient to describe the data. In the final model, mean CL was 0.124 L/h/kg0.75, V was 8.97 L/kg and bioavailability (F) was 12.5% (Tab.1). Inter-individual variability in CL, V and F was 57%, 104% and 61%, respectively. Covariate analysis suggested tacrolimus CL positively correlated with CrCL. Typical value of CL varied from 0.082-0.216 L/h/kg0.75 at the minimum and maximum CrCL values. Conclusion Routine therapeutic drug monitoring can be implemented in our dosage adaptation tool to assist with tacrolimus dosing in new paediatric SCT recipients. In future work, sample times for maximum information on an individual level will be evaluated using optimal design analysis. References 1. Antignac, M., et al., Population pharmacokinetics of tacrolimus in full liver transplant patients: modelling of the post-operative clearance. Eur J Clin Pharmacol, 2005. 61(5-6): p. 409-16. 2. Jacobson, P., et al., Factors affecting the pharmacokinetics of tacrolimus (FK506) in hematopoietic cell transplant (HCT) patients. Bone Marrow Transplant, 2001. 28(8): p. 753-8.






















