Download
1 / 1
10 likes | 194 Views
Barbara Reichetzer, Donna T Gilmour, Catherine Craig, Thomas Corkum, Robert F. Berry, Robert Abraham Dalhousie University, Halifax, NS, Canada. Preoperative Uterine Artery Embolization and Transvaginal Resection of Large Cervical Myomas. DISCUSSION

E N D
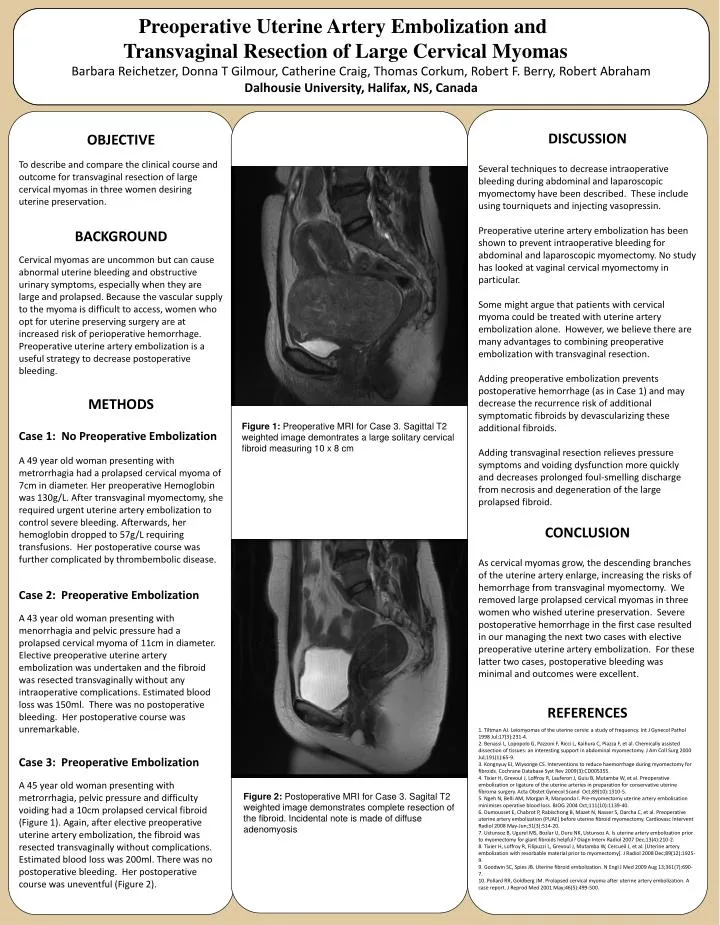
Barbara Reichetzer, Donna T Gilmour, Catherine Craig, Thomas Corkum, Robert F. Berry, Robert Abraham Dalhousie University, Halifax, NS, Canada Preoperative Uterine Artery Embolization and Transvaginal Resection of Large Cervical Myomas • DISCUSSION • Several techniques to decrease intraoperative bleeding during abdominal and laparoscopic myomectomy have been described. These include using tourniquets and injecting vasopressin. • Preoperative uterine artery embolization has been shown to prevent intraoperative bleeding for abdominal and laparoscopic myomectomy. No study has looked at vaginal cervical myomectomy in particular. • Some might argue that patients with cervical myoma could be treated with uterine artery embolization alone. However, we believe there are many advantages to combining preoperative embolization with transvaginal resection. • Adding preoperative embolization prevents postoperative hemorrhage (as in Case 1) and may decrease the recurrence risk of additional symptomatic fibroids by devascularizing these additional fibroids. • Adding transvaginal resection relieves pressure symptoms and voiding dysfunction more quickly and decreases prolonged foul-smelling discharge from necrosis and degeneration of the large prolapsed fibroid. • CONCLUSION • As cervical myomas grow, the descending branches of the uterine artery enlarge, increasing the risks of hemorrhage from transvaginal myomectomy. We removed large prolapsed cervical myomas in three women who wished uterine preservation. Severe postoperative hemorrhage in the first case resulted in our managing the next two cases with elective preoperative uterine artery embolization. For these latter two cases, postoperative bleeding was minimal and outcomes were excellent. • REFERENCES • 1. Tiltman AJ. Leiomyomas of the uterine cervix: a study of frequency. Int J Gynecol Pathol 1998 Jul;17(3):231-4. • 2. Benassi L, Lopopolo G, Pazzoni F, Ricci L, Kaihura C, Piazza F, et al. Chemically assisted dissection of tissues: an interesting support in abdominal myomectomy. J Am Coll Surg 2000 Jul;191(1):65-9. • 3. Kongnyuy EJ, Wiysonge CS. Interventions to reduce haemorrhage during myomectomy for fibroids. Cochrane Database Syst Rev 2009(3):CD005355. • 4. Tixier H, Grevoul J, Loffroy R, Lauferon J, Guiu B, Mutamba W, et al. Preoperative embolization or ligature of the uterine arteries in preparation for conservative uterine fibroma surgery. Acta Obstet Gynecol Scand Oct;89(10):1310-5. • 5. Ngeh N, Belli AM, Morgan R, Manyonda I. Pre-myomectomy uterine artery embolisation minimises operative blood loss. BJOG 2004 Oct;111(10):1139-40. • 6. Dumousset E, Chabrot P, Rabischong B, Mazet N, Nasser S, Darcha C, et al. Preoperative uterine artery embolization (PUAE) before uterine fibroid myomectomy. Cardiovasc Intervent Radiol 2008 May-Jun;31(3):514-20. • 7. Ustunsoz B, Ugurel MS, Bozlar U, Duru NK, Ustunsoz A. Is uterine artery embolization prior to myomectomy for giant fibroids helpful? Diagn Interv Radiol 2007 Dec;13(4):210-2. • 8. Tixier H, Loffroy R, Filipuzzi L, Grevoul J, Mutamba W, Cercueil J, et al. [Uterine artery embolization with resorbable material prior to myomectomy]. J Radiol 2008 Dec;89(12):1925-9. • 9. Goodwin SC, Spies JB. Uterine fibroid embolization. N Engl J Med 2009 Aug 13;361(7):690-7. • 10. Pollard RR, Goldberg JM. Prolapsed cervical myoma after uterine artery embolization. A case report. J Reprod Med 2001 May;46(5):499-500. OBJECTIVE To describe and compare the clinical course and outcome for transvaginal resection of large cervical myomas in three women desiring uterine preservation. BACKGROUND Cervical myomas are uncommon but can cause abnormal uterine bleeding and obstructive urinary symptoms, especially when they are large and prolapsed. Because the vascular supply to the myoma is difficult to access, women who opt for uterine preserving surgery are at increased risk of perioperative hemorrhage. Preoperative uterine artery embolization is a useful strategy to decrease postoperative bleeding. METHODS Case 1: No Preoperative Embolization A 49 year old woman presenting with metrorrhagia had a prolapsed cervical myoma of 7cm in diameter. Her preoperative Hemoglobin was 130g/L. After transvaginal myomectomy, she required urgent uterine artery embolization to control severe bleeding. Afterwards, her hemoglobin dropped to 57g/L requiring transfusions. Her postoperative course was further complicated by thrombembolic disease. Case 2: Preoperative Embolization A 43 year old woman presenting with menorrhagia and pelvic pressure had a prolapsed cervical myoma of 11cm in diameter. Elective preoperative uterine artery embolization was undertaken and the fibroid was resected transvaginally without any intraoperative complications. Estimated blood loss was 150ml. There was no postoperative bleeding. Her postoperative course was unremarkable. Case 3: Preoperative Embolization A 45 year old woman presenting with metrorrhagia, pelvic pressure and difficulty voiding had a 10cm prolapsed cervical fibroid (Figure 1). Again, after elective preoperative uterine artery embolization, the fibroid was resected transvaginally without complications. Estimated blood loss was 200ml. There was no postoperative bleeding. Her postoperative course was uneventful (Figure 2). Figure 1: Preoperative MRI for Case 3. Sagittal T2 weighted image demontrates a large solitary cervical fibroid measuring 10 x 8 cm Figure 2: Postoperative MRI for Case 3. Sagital T2 weighted image demonstrates complete resection of the fibroid. Incidental note is made of diffuse adenomyosis