Download
1 / 45
450 likes | 725 Views
The caBIG suite at UAMS. Umit Topaloglu Ph.D. Outline. Our goal The plan The current state of UAMS CTMS Our near future plans Research Billing Adverse Event capturing Conclusion. Our Goal. Is to create a clinical research informatics so:

E N D
The caBIG suite at UAMS Umit Topaloglu Ph.D.
Outline • Our goal • The plan • The current state of UAMS CTMS • Our near future plans • Research Billing • Adverse Event capturing • Conclusion
Our Goal • Is to create a clinical research informatics so: • Will be compliant with the federal and state regulation • Increase participant recruitment, • Cost saving • Solve research billing problems • Reduce time requirement for activating a study • Data integration towards personalized medicine and budgets are shrinking (including pharma)
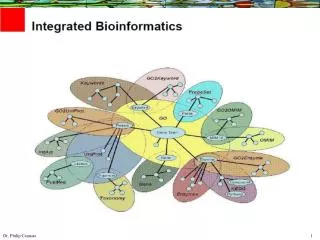
Clinical Research Informatics Infrastructure Utilizing open source and locally developed tools to create an interoperable clinical research informatics infrastructure. Most tools come from the NCI’s Cancer Biomedical Informatics Grid (caBIG). Open source applications are used when there is no caBIG tool available or a caBIG tool is insufficient. Developed in-house applications when no other tool existed.
Our needs for clinical research PLT – in house development Protocol/IRB tool- in house development Budgeting tool- in house development Recruitment- in house development Participant registry- C3PR Study Calendar- PSC Labs/grading- Labviewer/CALAEGS (CTCAE V3) CDMS- OpenClinica Adverse Event- In house/caAERS caTissue and caArray
Our approach Our approach is module by module to address our informatics needs. Due to: Minimize the adoption resistance. We started from most problematic areas Minimize the time required to implement all vs one (we have limited resource)
The Suite at UAMS Patient visits the Physician Cancer Central Clinical Participant Registry (C3PR v2) Patient Study Calendar (PSC) Tracks the patient schedule throughout the study Lab Viewer Eligibility is verified and patient is registered to a study caBIG Hub Identifies labs, loadsthem into the CDMSand AE system OpenClinica Cancer Adverse Event Reporting System (caAERS) CALAEGS CTCAE v3 Clinical data is captured Identifies and tracks adverse events and any associated schedule changes
C3PR-study and subject service We have More than 160 studies More than 2,000 participant registered. We also use in Psychiatric Research Institute National Children's Study College of Nursing
Patient Study Calendar Detailed study calendar It can manage; all the study related activities The same study structure with C3PR screening, treatment, follow up Activities imported from the IRB system with “R”, “C”, “I” to represent what account the activity should be charged.
caAERS Created an actual study and it is being tested Integration with labviewer and adverse event collection is planned
Labviewer Have done a proof of concept in version 1.5 In process of migrating to the new suite release CCHC has some problems We will import lab values using Mirth Connect
OpenClinica Electronic Data Capture and Clinical Data Management (CDM). 21 CFR Part 11 compliant (completed internally) Easy to setup even the most complicated studies. eCRF’s can be designed easily and support validations and calculations. Powerful discrepancy management functionality.
Common Data Elements for CRFs It is a mandate that all the CRFs has to have CDEs from caDSR in it. It is a time consuming commitment.
Other research data collection We have an online survey tool to let groups to create and publish questionnaire We use LimeSurvey open source tool Limesurvey is using UAMS sign in Cancer Control is harmonizing the surveys with CDE from caDSR. We‘ve completed Breast Moduler Mammography curation (~300 questions)
Reporting and Data Access LimeSurvey and OpenClinica have in built export functionality for statistical packages (R etc.) We use SQL Server Reporting Server for reports We can populate IRB Continuing Review Report automatically Other administrative reports
BioSpecimen/gene expression Management caTissue Suite 1.2 pulling registration from C3PR caArray for affymatrix and working on ilimuna Developed auto uploader/importer Implemented an interoperability scenario with caTissue
Data Quality • We have used Common Data Elements to help us clean population Science Data • Information Quality • Know what you have • Clean the existing • Prevent future repitition
Frequency analysis of the “RACE” category and basic analyses of the SSN
Current challenge- • Solve/minimize Research Billing problems • with the help of the Study Calendar. • Challenge • Complexity of issue • Terminology conversion
Steps and Challenges • Study budget is created using CPT codes • supposedly in calendar template • Convert CPT codes to SNOMED CT so clinic would understand • Office Visit is good example • Terminology conversion • Order/Billing using CPT • Another conversion back to CPT from SNOMED
Clinical Research Information flow Research orders Info from hospital Study details Study initiation Study conduct Enterprise Systems ET TrialSearch ADT (Healthquest) subject C3PR Centricity Calendar PSC Snomed SMS/ ChargeMaster LabViewer Approval SoftLab LABS OpenClinica
Research Billing Flow • 1- CLARA: Creating a comprehensive study patient care budget matrix 5) Verifying and coding the encounter form for compliance 2) Transfer the budget matrix into a patient study calendar template 4) Translating visit activities into an electronic encounter form 3) PSC: Tracking visits and recording visit activities
PSC messages PSC HL7 order 1- ICD-9 with safety codes(if applicable) HL7 order LAB, Radiology etc. EMR 1- activity performed 2- participant account number with plan code 3- charge type R, C, I, CNMS etc. Hospital and professional Billing
When we finish • We will know which research activities completed for which patient and where to be charge • Wrong charge research vs conventional problem will be solved.
Where are we • Technical implementation has been completed • Sending orders to EMR is live • Still working on lab workflow how/when to print specimen barcodes
Acknowledgement • People who contribute to the CTMS • Cheryl Lane • Jiang Bian PhD • Zhidan Feng • Saha Rinku • Samuel Jackson • Qiang Wang • Nitin Kanaskar • Vickie Chen • Emre Ermisoglu • Akheel Ahmed • Topeka Stacey • Bill O’Donnell • Ildeniz Yayla
Acknowledgement • Other Support • Cancer Institute • Peter Emanuel MD • Laura Hutchins MD • Thomas Kieber-Emmons PhD • Shirley Gray • Division of Biomedical Informatics • William Hogan MD • Shariq Tariq • CCTO • Sandy Annis • Chris Golden • Adam Hicks • Karen Mack • Missy McAdoo • UAMS Research Support Center • Grant Funding from Arkansas Breast Research Fund • Arkansas CCTR
Questions • Thanks for Listening • utopaloglu@uams.edu