Download
1 / 29
590 likes | 1.51k Views
ANTIARRHYTHMIC DRUGS. Arrhythmia/ dysrhythmia means an abnormal or irregular heart beat Arrhythmias may originate in the atria, SA node or AV node, whereby they are known as supra-ventricular arrhythmias or in the ventricles giving rise to the life-threatening ventricular arrhythmias.

E N D
ANTIARRHYTHMIC DRUGS • Arrhythmia/ dysrhythmia means an abnormal or irregular heart beat • Arrhythmias may originate in the atria, SA node or AV node, whereby they are known as supra-ventricular arrhythmias or in the ventricles giving rise to the life-threatening ventricular arrhythmias Causes of Arrhythmias • Arteriosclerosis • Coronary artery spasm • Heart block (mostly AV block) • Myocardial ischemia
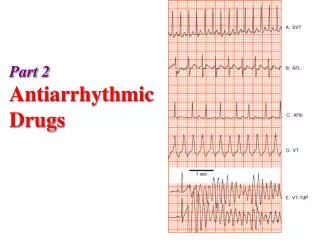
Specific Arrhythmias • Supraventricular Arrhythmias • Sinus tachycardia - high sinus rate of 100-180 beats/min as occurs during exercise or other conditions that lead to increased SA nodal firing rate • Atrial tachycardia - a series of 3 or more consecutive atrial premature beats occurring at a frequency >100/min; • Paroxysmal atrial tachycardia (PAT) of sudden onset, disappearance • Atrial flutter - sinus rate of 250-350 beats/min. • Atrial fibrillation - uncoordinated atrial depolarizations. • AV blocks - a conduction block within the AV node (or occasionally in the bundle of His) that impairs impulse conduction from the atria to the ventricles
Ventricular premature beats (VPBs) - caused by ectopic ventricular foci; characterized by widened QRS. • Ventricular tachycardia (VT) - high ventricular rate caused by aberrant ventricular automaticity or by intraventricular reentry; can be sustained or non-sustained (paroxysmal); characterized by widened QRS; rates of 100 to 200 beats/min; life-threatening. • Ventricular flutter - ventricular depolarizations >200/min. • Ventricular fibrillation - uncoordinated ventricular depolarizations
Pharmacologic Rationale & Goals • The ultimate goal of antiarrhythmic drug therapy: • Restore normal sinus rhythm and conduction • Prevent more serious and possibly lethal arrhythmias from occurring. • Antiarrhythmic drugs are used to: • decrease conduction velocity • alter the excitability of cardiac cells by changing the duration of the effective refractory period • suppress abnormal automaticity
Pharmacologic Rationale • Some drugs block fast sodium channels that determine how fast the membrane depolarizes (slope of phase 0, Vmax) & conduction velocity • Sodium channel blockers (Group I) reduce conduction velocity to abolish tachyarrhythmias caused by reentry circuits • Antiarrhythmic drugs affect cardiac refractoriness by changing ERP/APD via potassium channels and delay repolarization of action potentials (phase 3) • This would inhibit reentry tachycardias • Slow inward Ca channel blockers reduce SAnodal firing rate by slowing the rate of rise of depolarizing pacemaker potentials (phase 4 depolarization) • These drugs also reduce conduction velocity Ca-dependant tissue including the AV & SA nodal cells • Blockers of beta1-adrenoceptors can indirectly alter membrane ion conductance, particularly calcium and potassium conductance
ANTIARRHYTHMIC DRUGS • Most antiarrhythmic drugs are pro-arrhythmic • Only ß-blockers are proved to reduce mortality in post-myocardial infarction patients • They are classified according to Vaughan William into four classes according to their effects on the cardiac action potential
1. Class I ANTIARRHYTHMIC DRUGS Na+-ChannelsBlockers • Drugs in this class are blockers of voltage-operated fast Na+ channels in the myocardial membrane • They show (class IA & IB) preferential selectivity to Na+ channels in the open or inactivated closed states • Hence, they have better degree of blockade in tissues that are frequently depolarized or use-dependent or state-dependent • They decrease conduction velocity in non-nodal tissue (atrial and ventricular muscle, purkinje conducting system) • Group IA drugs have additionally moderate K+ channel blockade
Class IA DrugsQuinidine, Procainamide,Disopyramide • Class IA agents slow the phase 0/reduction of Vmaxof the cardiac action potential (conduction velocity) • They prolong muscle action potential & ventricular effective refractory period (refractoriness) • They decrease the slope of Phase 4 spontaneous depolarization, tending to suppress enhanced normal automaticity-induced arrhythmias
Class IA Drugs • They possess intermediate rate of association and dissociation with sodium channels • Pharmacokinetics: • Procainamide has good oral bioavailability • Procainamide is frequently used as IV slow route to avoid hypotension • Procainamide is metabolized into N-acetylprocainamide (NAPA), an active class III meatbolite mailnly cleared via the kidney, (dose adjustment in kidney failure) • Quinidine has good oral bioavailability & metabolized mainly in liver
Class IA Drugs Uses • Class IA drugs are effective in treatment of both supraventricular and ventricular arrhythmias • Quinidine rarely used for supraventricular arrhythmias • Oral quinidine/procainamide are used with class III drugs in refractory ventricular tachycardia patients with implantable defibrillator • IV procainamide used for hemodynamically stable ventricular tachycardia • IV procainamide used for acute conversion of atrial fibrillation including WPW syndrome
Class IA Drugs Toxicity Quinidine • A-V block at higher plasma levels • At toxic levels, ventricular tachycardia and torsade de pointes ventricular arrhythmia • Increasing digoxin plasma concentration by displacing digoxin from binding sites in addition to decreased digoxin renal clearance • Cinchonism occurs at large dose levels (blurred vision, tinnitus, headache, psychosis and gastrointestinal upset) • Digoxin is administered before quinidine to prevent the conversion of atrial fibrillation or flutter into paradoxical ventricular tachycardia. Quinidine shortens of A-V nodal refractoriness by atropine-like effects Procainamide • At high levels, asystole or induction of ventricular arrhythmias • Hypersensitivity reactions including drug fever and rarely agranulocytosis. • Systemic lupus erythromatosus (SLE)-like (arthralgia, fever & pleural-pericardial inflammation) • The SLE is dose- and time-dependent, and usually disappears upon drug stop • It is most common in patients with slow hepatic acetylation resulting in higher plasma level of the parent drug Disopyramide • 1. Anticholinergic side-effects • 2. Induction of ventricular arrhythmias in patients with prolonged QT interval • 3. Similar to quinidine, disopyramide may induce ventricular arrhythmia if used alone in the treatment of fibrillation
Class IB Drugs • They shorten Phase 3 repolarisation and decreases the duration of the cardiac action potential • They suppress arrhythmias caused by abnormal automaticity (c.f. quinidine suppresses enhanced normal automaticity-induced arrhythmias) • They show rapid association & dissociation with Na+ channels with appreciable degree of use-dependence
Agents of Class IB Lidocaine • It should be used by intravenous route because of its extensive first-pass metabolism • Lidocaine is the drug of choice in emergency treatment of ventricular arrhythmias Mexiletine and tocainide • These are the oral analogs of lidocaine • Mexiletine is used for chronic treatment of ventricular arrhythmias associated with previous myocardial infarction • Tocainide is used for ventricular tachyarrhythmias but its use is limited by its pulmonary toxicity that may lead to pulmonary fibrosis • Uses • They are used in the treatment of ventricular arrhythmias arising during myocardial ischemia or due to digoxin toxicity • They have little effect on atrial or AV junction arrhythmias
Class IC Drugs • They markedly slow Phase 0 fast depolarization • They possess slow rate of association and dissociation with sodium channels • They markedly slow conduction in the myocardial tissue • They only have minor effects on duration of action potential and refractoriness • They reduce automaticity by increasing the threshold potential rather than decreasing the slope of Phase 4 spontaneous depolarization
Class IC Drugs • Agents of Class IC: Flecainide & propafenone • Uses: • They are broad-spectrum but only approved for refractory ventricular arrhythmias • Flecainide is a particularly potent suppressant of premature ventricular contractions • Toxicity and Cautions for Class IC Drugs: • They are severe proarrhythmic drugs causing severe worsening of a preexisting arrhythmia or de novo occurrence of life-threatening ventricular tachycardia • In patients with frequent PVCs following MI, flecainide increased mortality compared to placebo • Notice: Class 1C drugs are particularly of low safety and have shown even to increase mortality when used chronically after MI
Class II ANTIARRHYTHMIC DRUGS(β-adrenergic blockers) • β-Adrenergic blockers produce both negative inotropic & chronotropic effects • They diminish phase 4 spontaneous depolarization suppressing automaticity and prolonging AV conduction Uses • They are used in treatment of increased sympathetic activity-induced arrhythmias such as stress- and exercise-induced arrhythmias • Treatment of atrial flutter and fibrillation • AV nodal tachycardia
Class II ANTIARRHYTHMIC DRUGS • Propranolol:was proved to reduce the incidence of sudden arrhythmatic death after myocardial infarction • Metoprolol & Pindolol • Metoprolol and other selective β1-adrenergic blockers reduce the risk of bronchospasm • Pidolol, having additional partial agonistic activity, may decrease the frequency of cardiac failure • Esmolol: • Esmolol is a very short-acting β1-adrenergic blocker that is used in the by intravenous route in acute arrhythmias occurring during surgery or emergencies
Class III ANTIARRHYTHMIC DRUGS • Class III antiarrhythmic drugs prolong phase 3 depolarization, without altering phase 0 upstroke or the resting membrane potential • They prolong both the duration of the action potential and the effective refractory period (ERP) • Their mechanism of action is still not clear but it is thought that they block potassium channels
Class III ANTIARRHYTHMIC DRUGS • Drugs of Class III: • Sotalol, bretylium, amiodarone, ibulitide • Uses: • They are used in the treatment of ventricular arrhythmias, especially ventricular fibrillation or tachycardia • Supra-ventricular tachycardia • Amiodarone usage is limited by its wide range of side effects
Class III ANTIARRHYTHMIC DRUGS Sotalol (Sotacor) • Sotalol is a β-adrenergic blocker that also prolongs the duration of action potential and refractoriness in all cardiac tissues • Sotalol suppresses Phase 4 spontaneous depolarization and possibly producing severe sinus bradycardia • The β-adrenergic blockade combined with prolonged action potential duration may of special efficacy in prevention of sustained ventricular tachycardia • It may induce the polymorphic torsade de pointes ventricular tachycardia Bretylium • It is generally administered parenteraly because of poor GIT absorption • Long-term oral use is associated with painful parotid enlargement as well as severe postural hypotension
Class III ANTIARRHYTHMIC DRUGSAmiodarone (Cordarone) • Amiodarone is a drug of multiple actions and not well understood • It is extensively taken up by tissues, especially fatty tissues, and has a half-life of up to 60 days • Amiodarone antiarrhythmic effect is complex comprising class I, II, III, and IV actions • Prolongation of action potential duration and refractoriness is the main • It slows cardiac conduction, works as Ca2+ channel blocker, and as a weak β-adrenergic blocker • Amiodarone Toxicity • Amiodarone has wide-spectrum toxicity • Most common include GI intolerance, tremors, ataxia, dizziness, hyper-or hypothyrodism • Corneal microdeposits may be accompanied with disturbed night vision • Other common side effects include liver toxicity, photosensitivity, gray facial discoloration, neuropathy, muscle weakness, and weight loss • The most dangerous side effect is pulmonary fibrosis which occurs in 2-5% of the patients
Class IV ANTIARRHYTHMIC DRUGS (Calcium Channel Blockers) • Calcium channel blockers decrease inward Ca2+ currents resulting in a decrease of phase 4 spontaneous depolarization • They slow conduction in Ca2+ current-dependent tissues like AV node • Verapamiland diltiazem, but not nifedipine (or the other dihydropyridine Ca2+ antagonists), are representative of this class being more effective on the heart than blood vessels
Class IV ANTIARRHYTHMIC DRUGS • Verapamiland diltiazem bind only to open depolarized voltage-operated Ca2+ channels, and hence preventing re-polarization until the drug dissociates from the channels. • Therefore, they are use-dependent blocking rapidly beating heart since in a normally-paced heart, Ca2+ channels have enough time to repolarize and the drug to dissociate from the channel before the next conduction cycle • Verapamiland diltiazem slow conduction and prolong effective refractory period in Ca2+ current-dependent tissues like AV node
Class IV ANTIARRHYTHMIC DRUGS • Verapamil& diltiazem are more effective in treatment of atrial than ventricular arrhythmias. • They are used in treatment of supra-ventricular tachycardia preventing the occurrence of ventricular arrhythmias • They are used in treatment of atrial flutter and fibrillation • Both drugs are contraindicated patients with pre-existing depressed heart function because of their negative inotropic activity • Both drugs may cause bradycardia, and asystole especially when given in combination with β-adrenergic blockers
Miscellaneous Antiarrhythmic Drugs Adenosine • Adenosine activatesA1-purinergic receptors decreasing the SA nodal firing and automaticity, reducing conduction velocity, prolonging effective refractory period, and depressing AV nodal conductivity • It is the drug of choice in treatment of paroxysmal supra-ventricular tachycardia • It is used only by slow intravenous bolus • It has only low-profile toxicity being ultra-short acting of 15 seconds duration
Compare between class IA, IB, and IC drugs as regards effect on Na+ channel & ERP • Sodium-channel blockade: IC > IA > IB • Increasing the ERP:IA>IC>IB (lowered)