Download
1 / 109
1.13k likes | 1.67k Views
Antiarrhythmic Drugs. Paul Miller, Pharm.D. Emergency Clinical Pharmacy Specialist St. Elizabeth Health Center August 2012. Overview. Brief arrhythmia pathophysiology review Antiarrhythmic medications Mechanism Use Dosing Clinical pearls Use in the Emergency Department Discussion.

E N D
Antiarrhythmic Drugs Paul Miller, Pharm.D. Emergency Clinical Pharmacy Specialist St. Elizabeth Health Center August 2012
Overview • Brief arrhythmia pathophysiology review • Antiarrhythmic medications • Mechanism • Use • Dosing • Clinical pearls • Use in the Emergency Department • Discussion
Arrhythmia pathophysiology • “Arrhythmias result from abnormalities of impulse initiation or impulse conduction, or a combination of both”1
Impulse formation disturbances • Can be no pathological change in pacemaker sites • Sinus Bradycardia (<60bpm) – slowed SA node impulse formation • Sinus Tachycardia (>100bpm) – rapid SA node impulse formation • Ectopic focus • Impulse generated outside SA node • Electrolyte disturbances, ischemia, excessive myocardial stretch, drugs, toxins Williams & Wilkins, 2011
Conduction abnormalities • Most common conduction abnormalities involve conduction blocks (Heart block) • Usually caused by localized or regional hypoxia from decreased coronary blood flow • Hypoxia decreases action potential amplitude and rate of depolarization (phase 0 slope) • Areas of conduction block can lead to reentry circuits (major cause of ventricular and supraventricular tachyarrhythmia's) Williams & Wilkins, 2011
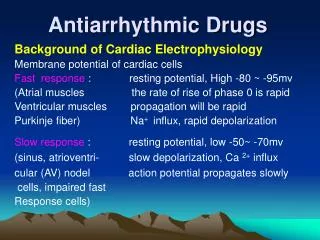
SA and AV node action potentials • Pacemaker cells • No true resting potential (phase 4) • Unlike other cells, the depolarizing current enters the cell via slow Ca++ currents, rather than Na currents • Slow response action potentials Williams & Wilkins, 2011
SA and AV node action potentials Williams & Wilkins, 2011
Non-pacemaker action potentials • Atrial myocytes, ventricular myocytes and Purkinje cells • Rapid depolarization “fast response” • Phase 0 – Na • Phase 1 – K • Phase 2 – Ca • Phase 3 – K Williams & Wilkins, 2011
Conversion to pacemaker cells • Non-pacemaker cells can undergo spontaneous depolarizations under certain conditions • Hypoxia causes membrane depolarization, which closes fast Na channels • Inward Ca++ current can initiate spontaneous action potentials and automaticity • Mechanism for ectopic beats and arrhythmias seen in ischemic heart disease patients Williams & Wilkins, 2011
Assessment question • Slow Ca++ channels are responsible for membrane depolarization in which type of tissue/cells? • A. Ventricular myocytes • B. Atrial myocytes • C. SA/AV nodal cells • D. Skeletal muscle cells
Effective Refractory Period (ERP) • Period of time a new action potential can NOT be initiated • Protective mechanism to limit rapid successive depolarization (and HR) • Many antiarrhythmic drugs alter the ERP • Altering (prolonging) the ERP can be effective for abolishing reentry currents Williams & Wilkins, 2011
Reentry • Most common mechanism for most tachyarrhythmia's • For reentry to occur, 3 conditions must be met • Unidirectional block • Critical timing • Length of block matches refractory period Williams & Wilkins, 2011
Reentry Williams & Wilkins, 2011
Global Reentry (SVT and WPW) Williams & Wilkins, 2011
Assessment Question • What are the 3 requirements for a reentry circuit to occur?
Assessment Question • What are the 3 requirements for a reentry circuit to occur? • 1. Unidirectional block • 2. Critical timing • 3. Length of block matches refractory period
Antiarrhythmic drug classification • Vaughan Williams • Class I – Na channel Blockers • Class II – Beta Blockers • Class III – K channel blockers • Class IV – Ca channel blockers • Miscellaneous • Atropine, Adenosine, Digoxin, Electrolytes (Mag, K), Williams & Wilkins, 2011
Class I – Na Channel Blockers • !a: Quinidine, Procainamide, Disopyramide • 1b: lidocaine, mexiletine • 1c: Flecainide, Propafenone, • All block fast sodium channels responsible for depolarization (phase 0) of non-nodal action potentials • Decreased slop of phase 0 • Remember: non-nodal = Atrial and ventricular myocytes and purkinje cells • Nodal cells cells of the SA node and AV node (depolarization occurs by Cachannels) Williams & Wilkins, 2011
Class I – Na Channel Blockers • By decreasing slope of phase 0, Class I drugs can interrupt conduction in reentry circuits (a good thing) • Differences in Na channel blockade and ERP • Class 1a: Moderate blockade • Increase ERP • Class 1b: Weak • Decrease ERP • Class 1c: Strong • No change ERP Williams & Wilkins, 2011
Class Ia Williams & Wilkins, 2011
Class 1a: Procainamide • Stable monomorphic ventricular tachycardia • Dose: 100mg IV every 5 minutes until arrhythmia controlled, hypotension occurs, further QRS widening, up to total 17mg/kg • Then start infusion 1-4mg/min. • Note: Not recommended for Vfib or hemodynamically unstable Vtachdue to long administration times and unknown efficacy • If known hepatic impairment, reduce dose by half • After conversion to sinus rhythm, possible tachycardia from anticholinergic effects after prolonged administration Coyle, 1992
Class Ia • Quinidine rarely used due to newer more effective treatments • Disopyramide • Oral Class 1a antiarrhythmic • Only used for last line therapy due to adverse effects and newer more effective treatment • Negative inotropic effects. Do not use in patients with LVEF < 40% • Strong anticholinergic activity Coyle, 1992
Class 1b Williams & Wilkins, 2011
Lidocaine – Class 1b • Weak inhibitor of fast sodium channels in non-nodal cardiac myocytes • Decreases ERP • Hemodynamically stable Vtach • 1-1.5mg/kg (usually 100mg syringe) IV x 1 bolus, then continuous infusion 1-4mg/min (usually 1mg/min) • Can repeat 0.5-0.75mg/kg bolus as necessary. • Usually second line to amiodarone • Caution lidocaine toxicity with prolonged infusions • Consider use for Vfib refractory to shock and amiodarone Dorian 2002
Mexiletine – Class 1b • Orally active analog of Lidocaine • Not used for termination of active ventricular arrhythmia, should use IV lidocaine • Most commonly used to prevent serious ventricular arrhythmias in patients with pacemaker • Can load 400mg PO, then 200mg every 8 hours (if converting from IV procainamide) or start at 200mg every 8 hours (if converting from IV lidocaine) • Start 6-8 hours after stopping IV lidocaine Williams & Wilkins, 2011
Class 1c Williams & Wilkins, 2011
Flecainide • Oral Class 1c anti-arrhythmic • No utility in the ER • Contraindicated in CAD (CAST trial) • BEERS list for anti-cholinergic effects • Used to prevent life threatening ventricular arrhythmias or PSVT. • Also used as “Pill-in-the-pocket” • 200mg PO x1 (<70kg), 300mg PO x1 (>70kg) for palpitations • Reduced ER visits by 94% (Alboni 2004) • Only for select patients with infrequent paroxysmal Afib Alboni 2004
Propafenone • Oral class 1c antiarrhythmic • Prevent recurrence of Afib • 225mg PO q12 hr • Pharmacologic cardioversion (unlabeled use) • 600mg PO x 1 dose • To prevent rapid AV conduction, patients should be initiated on beta blocker or non-DHP calcium channel blocker prior to initiating therapy • Also a BEERS medication Williams & Wilkins, 2011
Class II antiarrhythmics – Beta-Blockers • MOA: Bind to beta-adrenergic receptors and block the activity of epinephrine and norepinephrine • Inhibits normal sympathetic effects through these receptors • “Partial Agonists” • Provide some background sympathetic activity while preventing normal enhanced sympathetic activity • “intrinsic sympathomimetic activity” (ISA) • Membrane stabilizing activity (MSA) (ex. Metoprolol) Williams & Wilkins, 2011
Beta-Blockers • First generation = non-selective • Block both Beta-1 and Beta-2 adrenergic receptors • Second generation = relative Beta-1 selectivity • Cardioselective • Beta-1 selectivity overcome by higher doses • Third generation = additional alpha blocking properties • Vasodilation effects through alpha-1 blockade • Mainly used for HTN Williams & Wilkins, 2011
Beta Blockers • Actions on cardiac tissue • Block beta receptors in nodal tissue, conducting system, and contracting myocytes • Predominantly beta-1 receptors in cardiac tissue • Beta-2 receptors more predominant in airway smooth muscle • Caution COPD and asthma Williams & Wilkins, 2011
Beta-blockers for arrhythmia • Normal sympathetic influences on cardiac electrical activity • Increased SA node automaticity (pacemaker activity) – increased sinus rate • Increased conduction velocity at AV node • By decreasing conduction velocity beta-blockers abort reentry circuits • Beta-blockers also affect non-pacemaker action potentials • Increase APD and ERP • Again effective for treating reentry circuits Williams & Wilkins, 2011
Metoprolol • Selective beta-1 blocker • Decreases rate of depolarization in nodal tissue • Afib, SVT rate control: 2.5-5mg IVP every 3-5 minutes up to maximum 15mg in 15 minutes • Only use if hemodynamically stable • Caution decompensated heart failure • Contraindicated Wolff Parkinson White (WPW) syndrome Williams & Wilkins, 2011
Other beta blockers • Labetalol • Beta-1 and beta-2 blockade and alpha-1 blockade • Solely used for HTN, not arrhythmia • Other selective beta-1 blockers similar to metoprolol, however metoprolol primary class II anti-arrhythmic. • Why not Sotalol? Actually classified as Class III anti-arrhythmic Williams & Wilkins, 2011
Class III anti-arrhythmics • K+ channel Blockers • K+ channels responsible for cell repolarization • Work both in nodal and non-nodal tissue • After Na+ and Ca++ channels are activated, K+ channels begin to open • Allows K+ to leave cell, causing membrane potential repolarization • Repolarize fast response action potentials in non-nodal tissue • Repolarize slow response action potentials in nodal tissue Williams & Wilkins, 2011
Class III anti-arrhythmics Williams & Wilkins, 2011
Class III anti-arrhythmics • Blocking K+ channels slows or delays membrane repolarization • Increased action potential duration (APD) • And increased effective refractory period (ERP) • On the EKG, this will prolong QT interval • Classic effect of all class III anti-arrhythmics • Prolongs the time the cell is not excitable • By increasing the ERP – very useful for terminating reentry mechanisms Williams & Wilkins, 2011
Amiodarone • Uses: Vtach, Vfib, rate control in Afib/flutter • Has activity of all Classes of antiarrhythmics, mostly K+ blockade • Extremely long T1/2 – 45-60 DAYS! • Lots of drug interactions including Warfarin • Warfarin adjustments needed for up to several months • Lots of side effects Williams & Wilkins, 2011
Amiodarone side effects • Lungs • Interstitial pneumonitis • Pulmonary fibrosis • Thyroid (iodine component) • Structurally similar to T4 • Eyes • Corneal deposits in 90% of patients after 6 months • Usually asymptomatic • GI/Liver toxicity • Skin – UV sensitivity • Hands/Feet – neuropathy Williams & Wilkins, 2011
Amiodarone dosing • Stable Vtach: 150mg/100mL over 10 minutes followed by continuous infusion 1mg/min x 6hrs then 0.5mg/min • SVT: 150mg/100mL over 10 minutes • Afib RVR: 150mg/100mL over 10 minutes, then 1mg/min • Vfib /pulseless vtach(ACLS) refractory to defibrillation: 300mg IV push, may repeat 150mg Iv push after 3-5min. If ROSC occurs, initiate continuous infusion • If they are Pulseless, then Push it! Williams & Wilkins, 2011
Dronedarone • Structurally very similar to amiodarone without iodine • Developed as alternative to amiodarone • Lacks side effects of amiodarone (pulmonary thyroid) • Increased mortality in patients with heart failure (ANDROMEDA 2007) • PALLAS trial 2011 – double risk of cardiovascular death in patients with permanent Afib. Williams & Wilkins, 2011
Sotalol (Betapace) • Non-selective beta blocker, also K+ channel blocker • Dual action – prolongs both PR interval and QTc interval • Use for stable Vtach (unlabeled) and prevention of Afib • Dose: (Stable monomorphic Vtach) 1.5mg/kg over 5 minutes (ACLS 2010) • Must monitor renal function and QTc Williams & Wilkins, 2011
Dofetilide (Tikosyn) • Oral Class III anti-arrhythmic • Dose related increases in QTc • Must be initiated in hospital with constant EKG monitoring • Remember! Drug interactions and QTc prolongation! • Avelox, Zofran, Geodon all contraindicated • Renally cleared • Must be T.I.P.S. certified to prescribe Williams & Wilkins, 2011
Class IV anti-arrhythmics • Ca++ channel blockers • Only non-dihydropyridine Ca++ channel blockers • Diltiazem and Verapamil • Block Ca++ channels in cardiac Nodal tissue, also causes peripheral vasodilation • Slows conduction through AV node, increases time needed for each beat, decreased myocardial oxygen demand, effective for reentry supraventricular tachycardias • Negative inotropic effects • Contraindicated in decompensated heart failure Williams & Wilkins, 2011
Diltiazem (Cardizem) • Use: Angina, HTN, rate control in Afib/flutter, PSVT • Dose (Afib rvr): 0.25mg/kg IV slow push (ACLS recommends 15-20mg) • 10mg often used, but is a wussy dose! • May repeat 0.35mg/kg (ACLS recommends 20-25mg) after 15 min • Initiate infusion at 10mg/hr • Titrate to desired HR (15mg/hr max) • Many patients respond to 5mg/hr Williams & Wilkins, 2011
Diltiazem (Cardizem) • Only for hemodynamically stable patients • Contraindicated SBP<90, cardiogenic shock, administration within 2 hours of IV beta blocker • Also contraindicated in Afib/flutter associated with accessory bypass tract (WPW) • Conversion to PO • Oral dose (mg/day) = [rate(mg/hr)x3 +3] x 10 • 3mg/hr = 120mg/day • 5mg/hr = 180mg/day • 7mg/hr= 240mg/day • 11mg/hr = 360mg/day Williams & Wilkins, 2011
Assessment Question • Which VW class antiarrhythmic slow conduction velocity and depolarization in Non-Nodal tissue (Ventricular/Atrial myocytes, Purkinje cells)? • A. Class I • B. Class II • C. Class III • D. Class IV
Assessment Question • Before prescribing Avelox (moxifloxacin), what antiarrhythmic should you make sure the patient is NOT taking?