Download
1 / 68
1.46k likes | 3.44k Views
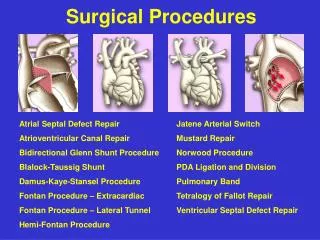
Jamal Al-Asiri. Surgical Approaches. The Foot. Fore foot: Medial approach to MT1 Dorsal approach to MT1 Dorsal intermetatarsal approach Mid foot: Dorsal double parallel incisions. Foot: 1 st MTP Joint ( Dorsomedial & Dorsal). Indications

E N D
Jamal Al-Asiri Surgical Approaches
The Foot • Fore foot: • Medial approach to MT1 • Dorsal approach to MT1 • Dorsal intermetatarsal approach • Mid foot: • Dorsal double parallel incisions
Foot: 1st MTP Joint (Dorsomedial & Dorsal) • Indications • Bunionectomy, DSTP, Osteotomies, Arthroplasty, Fusion • Position • Supine + Tourniquet • Landmarks/Incision • MT Head + EHL • Dorsomedial • Direct medial over MTP joint • Medial to EHL • Plantar to dorsal digital nerve • Parallel to Phalanx distal and MT shaft proximal • Dorsal • Medial to EHL • Directly over MTP joint • Inline with the phalanx + shaft • Plane • None
Foot: 1st MTP Joint (Dorsal & Dorsomedial) • Superficial • Dorsomedial • Incise deep fascia inline • Directly down to MTP joint • Retract EHL + Dorsal Digital nerve • Dorsal • Incise deep fascia inline • Retract EHL Lateral • Directly down to MTP joint • Deep • Reflect periosteum off phalanx + MT • Dangers • EHL • Dorsal digital nerve • FHL (too much phalanx stripping plantar side) • Deep Peroneal Nerve (1stwebspace)
Dorsal double parallel incisions • Positioning • supine, with a bump under the affected hip. • Incisions: • The first incision is longitudinal, in the space between first and second MTs or over the second MT. • It is approximately 5 cm in length, lateral to the extensor hallucis longus (EHL), with the distal end of the incision 3 cm distal to the first TMT joint. • The superficial sensory branches of the superficial peroneal nerve are isolated and preserved. • The inferior extensor retinaculum is excised, and the neurovascular bundle found between the EHL and EHB is isolated. The EHL is retracted medially to visualize the Lisfranc joint. • If the third TMT joint is still unstable, a second longitudinal incision is created over the third-fourth MT space or over the fourth MT. • The lateral superficial sensory branches of the superficial peroneal nerve are protected. • The (EDL) is elevated to expose the (EDB), which can be split longitudinally or elevated from lateral to medial.
The Foot • Hind foot (Talus): • Anterolateral to the talus • Anteromedial to the talus • Posteromedial to the talus • Posterolateral to the hindfoot
Anteromedial Approach to the Talus • Postion: • Supine • Incision: • 10cm longitudinal curved incision on the medial aspect of the ankle just anterior to the tip of the medial mal • Interval: • Between Tib ant& Tib post • Dangers: • Saphenous nerve and long saphenous vein
Anterolateral Approach to the Talus • Postion: • Supine with sandbag under the hip • Incision: • 10 cm slightly curved incision on the anterolateral aspect of the ankle 2cm anterior to the anterior border of the fibula, toward the base of the 4th metatarsal • Interval: • Peroneal muscles (superficial peroneal nerve) and extensor muscles (deep peroneal nerve); Detach and reflect the extensor digitorumbrevis from it origin on the calcaneus • Dangers: • Dorsal cutaneous branches of superficial peroneal n.; Deep peroneal n. & dorsalispedis art
Posteromedial approach to the talus Anatomy This rarely-used approach is extremely useful and follows the plane between flexor hallucis longus and the Achilles tendon. The neurovascular structures lie posteromedially behind the medial malleolus and must be protected Incision Skin incisionUsing the Achilles as the lateral boundary, and the neurovascular structures posteromedially, a skin incision is made centered over the subtalar joint using image intensification.
Posteromedial approach to the talus Superficial dissectionThe structures that run behind the medial malleolus are very important here. The most posterior structure, flexor hallucis longus, is identified so the surgeon can go posterior and lateral to it and medial to the Achilles tendon. Deep dissectionThe tendon sheath of the flexor hallucis longus must be opened. This allows the retraction of the tendon together with the neurovascular bundle and gains exposure of the fracture.Lateral to the tendon sheath of the FHL is the posterior tubercle of the talus.The surgeon must be careful not to be too proximal and mistake the distal tibia for the talus. Fixation and debridement can now be completed.
Posterolateral approach to the talus Incision This approach is very useful as it is a true internervous and intermuscular approach which is very safe. It is useful as an approach to the posterior talus, the posterior aspect of the distal tibia, the posterior distal fibula and the posterior portion of the calcaneus.The skin incision is made vertically between the peroneal tendons anteriorly and the Achilles tendon posteriorly. In the depth one encounters the sural nerve which must be protected together with its lateral calcaneal branch, which - if cut - results in a painful neuroma. Deeper and medially one encounters the belly of the flexor hallucis longus. For an approach to the talus and the subtalar joint and the Volkmann’s triangle the flexor hallucis longus must be retracted medially.
The Foot • Hind foot (Calcaneus): • Extended lateral approach to calcaneus • Medial approach to the calcaneus
Extended lateral approach to calcaneus Anatomy Vascular supply The perforating branches of the peroneal artery contribute to the vascularity of the lateral skin and soft tissue of the foot. The undermining of skin edges runs the risk of skin edge necrosis and therefore full-thickness flaps have to be developed to prevent this complication. The lateral calcaneal artery is responsible for the majority of the blood supply to the corner of the L-shaped flap of this approach. The heel pad is mostly supplied from the posterior tibial artery branches medially.The sural nerve needs to be protected in the horizontal part of the approach.
Extended lateral approach to calcaneus Incision Skin incisionThe posterior arm of the incision is placed midway between the fibula and Achilles tendon. The horizontal arm is placed in line with the base of the fifth metatarsal.They meet at a corner where skin handling must be optimized. Development of flapThe undermining of the edges must be avoided. One creates a full-thickness flap and, as the flap is developed, one divides the retinaculum and detaches the CFL and talocalcaneal ligaments from bone. The peroneal tendons and the sural nerve are within the flap and are not exposed. As the flap is developed upwards, one exposes the subtalar joint and the sinus tarsi.
Extended lateral approach to calcaneus Incision Skin incisionThe posterior arm of the incision is placed midway between the fibula and Achilles tendon. The horizontal arm is placed in line with the base of the fifth metatarsal.They meet at a corner where skin handling must be optimized. Development of flapThe undermining of the edges must be avoided. One creates a full-thickness flap and, as the flap is developed, one divides the retinaculum and detaches the CFL and talocalcaneal ligaments from bone. The peroneal tendons and the sural nerve are within the flap and are not exposed. As the flap is developed upwards, one exposes the subtalar joint and the sinus tarsi.
Medial approach to calcaneus Incision Skin incisionThe center of the incision is 2 cm beneath the medial malleolus and 2 cm proximal to the navicular.To achieve adequate visualization of the sustentaculum, it needs to be about 5 cm in length, following the neurovascular structures. Superficial dissectionOnce beneath skin, identify the posterior tibial tendon, the neurovascular bundle and the flexor hallucis tendon. The interval to develop is between the neurovascular bundle, specifically the posterior tibial nerve and the flexor hallucis tendon, which is retracted distally.
Medial approach to calcaneus Deep dissectionThe sustentaculum is a bony prominence which is obvious once one is beneath the medial neurovascular structures. Usually, fixation is placed into the calcaneus immediately below the sustentaculum, which has been fractured and displaced plantarwards. Image intensification will verify the surgeon’s position in this deep approach.The small bony fragment mandates use of mini fragment fixation.
The Ankle • Lateral approach • Medial approach • Posterolateral approach** • Posteromedial approach • Anterior approach
Lateral approach Incision If a lateral plate is required for the lateral malleolus, the incision should be placed either slightly anteriorly or posteriorly, so that the plate does not come to lie directly beneath the incision. If a posterior plate is planned, place the incision slightly posteriorly, so that the soft-tissue dissection can be minimized. Proximal extension In case a distal fracture extends proximally, the incision can be extended proximally. The plane of dissection is the same, but particular care must be taken with the superficial peroneal nerve. In this case it is advisable to identify and protect the nerve.
Lateral approach Superficial surgical dissection The dissection plane is between the peroneus tertius anteriorly and the peroneus longus and brevis posteriorly. The figure shows a long incision, such as would be used for suprasyndesmotic fractures. Handling the damaged soft tissue is crucial. Use small retractors only in good soft-tissue conditions. Retracting with protecting sutures is a safe method. NoteBe careful not to damage the superficial peroneal nerve, which lies very closely anteriorly, especially in the proximal part of the incision. In more anterior incisions, it should be identified and protected. When dissecting posteriorly, be careful not to damage the short saphenous vein and the sural nerve.
Lateral approach Deep surgical dissection Free the periosteum at the fracture site. In order to minimize devascularization, reflect only as much of the periosteum as is needed to expose the fracture site. Unnecessary stripping of the periosteum reduces the blood supply of the bone. If it is necessary to extend the dissection, keep it close to the periosteum, in order to avoid damage to terminal branches of the peroneal artery. The fracture site is now exposed and should be cleaned before it is reduced.
Medial approach Incision Start the incision 2 cm distal to the anterior tip of the medial malleolus. Curve the incision towards the anterior edge of the medial malleolus and in the direction of the middle of the distal tibia. Find the saphenous vein and nerve, and use a vessel loop to retract them. Surgical dissection Expose the anterior part of the fracture site, free the periosteum from the edges of the medial malleolus to the distal tibial joint surface and inspect the joint. If necessary, make a vertical incision at the anteromedial edge of the joint capsule. Dissect the capsule as far as necessary to visualize the fracture and the joint surfaces. Remove the periosteum posteriorly only sufficiently to control reduction.
Posteromedial approach Incision This approach is indicated in cases of posterior comminution and/or a posterior extension of a medial malleolar fracture. Start the incision 1 cm distal and 1 cm anterior to the middle of the tip of the medial malleolus. Curve the incision dorsally over the tip of the medial malleolus and in the direction of the posterior crest of the distal tibia. NoteBe careful not to damage the saphenous vein and nerve, especially distally. Superficial surgical dissection Deepen the approach through the subcutaneous fat and the fascia, in a direct line with the posteromedial crest of the tibia. Deepen the dissection of the fracture site without stripping off the periosteum.
Posteromedial approach Deep surgical dissection Follow the fracture line to the posterior edge of the distal tibia. Open the crural fascia at the edge of the posterior tibia, proximally as far as necessary, and distally as far as the proximal insertion of the flexor retinaculum. Retract the tendons of the tibialis posterior muscle and the flexor digitorum longus muscle and the posterior tibial neurovascular bundle, using blunt retractors. Develop the dissection until the fracture line at the posterior part of the tibia is entirely in view. Dissect the periosteum only as far as required for the control of the reduction at the metaphysis. If necessary, follow the fracture line anteriorly. Protect the saphenous nerve and vein.
Tibia/Fibula • Distal Tibia: • Anteromedial approach • Anterolateral approach • Posteromedial approach • Posterolateral approach
Anteromedial approach Skin incision The incision for the anteromedial approach starts about 5–8 cm proximal to the ankle joint, lateral to the tibial crest. It runs in a straight line over the ankle joint towards the base of the navicular, following the medial border of the anterior tibial tendon. A straight incision provides a better approach to the anterior part of the tibia than a curved incision.
Anteromedial approach Surgical dissection Deepen the dissection to the periosteum along the medial border of the anterior tibial tendon, leaving the tendon sheath intact. Minimal exposure and careful handling of the periosteum are essential to prevent any further vascular damage of the fracture fragments. The tibiotalar joint is opened in the sagittal direction, usually in line with the fracture line between the two main anterior articular fragments. Any transverse incision of the anterior capsule to further expose the joint should be kept short as this risks devascularization of the anterior fragments (supplied by branches of the anterior tibial artery).
Anterolateral approach Skin incision This incision is centered at the ankle joint, parallel to the fourth metatarsal distally, and parallel to and between the tibia and fibula proximally. Dissection through the skin and subcutaneous tissues should proceed sharply with maintenance of full thickness skin flaps. Since the anterior compartment muscles arise from the anterior fibula, the incision is usually not extended more than seven centimeters above the ankle joint. Distally, the incision can extend as far as the talonavicular joint. SPN Take care not to damage the superficial peroneal nerve which lies directly beneath the skin. This nerve invariably crosses the surgical incision proximal to the ankle joint. It should be identified, mobilized, and protected throughout the surgical procedure.
Anterolateral approach Surgical dissection Distally, the extensor retinaculum is incised and the anterior compartment tendons are all retracted medially. Proximally, the entire anterior compartment musculature, including the peroneus tertius, can then be mobilized and retracted medially. The fascia of the extensor digitorum brevis can be incised, with the muscle carefully dissected and retracted medially. This allows exposure of the talar neck for pin placement and distractor application. Proper location of the arthrotomy, preplanned to lie over the fracture, is critical to avoid unnecessary and damaging devascularization of fracture fragments. Proximally, the dissection is limited by the origin of the anterior compartment muscles from the fibula and from the interosseous membrane.
Posteromedial approach Incision The incision is centered at the ankle joint, between the Achilles tendon and the posteromedial border of the distal tibia. Proximally the incision parallels the posteromedial border of the tibia. Distally the incision parallels the path of the posterior tibial tendon. Superficial surgical dissection Deepen the incision through the subcutaneous fat and fascia and reveal the deep fascia over the tendons of tibialis posterior and flexor digitorum longus, the posterior tibial neurovascular bundle and the flexor hallucis longus tendon. For access to the posteromedial quadrant of the distal tibia, it is necessary to carefully incise the deep fascia proximally, protecting the neurovascular bundle.
Posteromedial approach Deep dissection The interval used for deep dissection is dependent on the location of the major fracture fragments. 1) It may be between the tibia and the posterior tibial tendon. This is useful for proximal exposure only as the distal posterior tibial tendon should not be dissected from the posterior tibia. 2) It may also be between the posterior tibial tendon and the flexor digitorum communis (see illustration). (2) (3) 3) Or it may be between the flexor digitorum comminus and the flexor hallucis longus. The latter of these three intervals requires direct exposure and protection of the neurovascular bundle along its length. The neurovascular bundle can be retracted anteromedially or posterolaterally.
Posterolateral approach Skin incision Skin incision is made along the posteromedial border of the fibula and can extend from the tip of the fibula as far proximally as is required. It should never be more medial than the lateral border of the Achilles tendon. Protect the sural nerve It is important to be aware of the course of the sural nerve as it courses from the center of the calf proximally to just posterior to the fibula distally. Identify the sural nerve under the superficial fascial layer and usually include it in the lateral flap. If the dissection is extended more proximally, it may be necessary to work on either side of this nerve.
Posterolateral approach Exposure of the fibula Superficial surgical dissection to the fibula If the fibula requires fixation, this option is chosen. Maintain full thickness superficial flaps to reduce the risk of skin necrosis. Superficial dissection should be taken down to the attachment of the peroneal fascia on the posterolateral border of the fibula. Incise the fascia, and retract the peroneals medially.
Posterolateral approach Approach to the tibia Surgical dissection to the tibia Access to the tibia is through a separate plane which is developed on the posteromedial border of the peroneal muscles. These are now retracted laterally. Exposure of the posterior aspect of the tibia is achieved by developing the interval between the peroneal tendons and muscles laterally and the flexor hallucis longus (FHL) medially.
Posterolateral approach Deep surgical dissection to the tibia FHL is recognizable from the very distal extent of its muscle belly. It can also be identified by moving the great toe. With sharp dissection of the FHL along its lateral border, the entire posterior aspect of the tibial surface can be exposed by retracting this muscle medially. This also provides protection of the posteromedial neurovascular bundle. Tibia: Exposure of the joint surface Visualization of the articular surface or small fragments preventing reduction of the articular pieces can be difficult. The posterolateral fragment is rotated laterally around the usually intact posterior tibiofibular ligament. The interval between the boney fragments is developed giving access to the center of the fracture.
Tibia/Fibula • Tibia shaft: • Anteromedial approach • Anterolateral approach • Posteromedial approach • Posterolateral approach
Anteromedial approach Skin incision Approach the anteromedial surface through a longitudinal incision 1-2 cm lateral to the tibial crest. Distally, continue along the medial edge of the tibialis anterior in a gentle curve in the direction of the medial malleolus. The deep dissection should stay superficial to the fascia layer of the anterior compartment. The length of the incision depends on the planned plate length. Take care not to compromise the saphenous vein and nerve, which are at risk at the distal extend of the approach.Entrance into the anterior tibial tendon sheath should be avoided, as this can cause unwanted adhesions.
Anteromedial approach Dissection Full thickness skin and subcutaneous tissue flaps are then mobilized in a medial direction. In this way the anteromedial aspect of the tibia is directly exposed. The periosteum is left intact, or minimally reflected from the fracture edges, if necessary for a direct anatomical reduction.
Anterolateral approach Skin incision A longitudinal incision lies 1-2 cm lateral to the tibial crest and continues distally straight over the ankle joint along the line of the anterior tibial tendon. The length of the incision depends on the plate length. The distal extension of the anterolateral approach is helpful for distal tibial fractures, but is obstructed by muscles and neurovascular structures of the anterior compartment.
Anterolateral approach Dissection The fascia is incised just lateral to the tibial crest and the dissection is carried down extraperiostally along the lateral surface of the tibia. The periosteum is left intact, though it may require mobilization near the fracture site for exposure of fracture edges. This is commonly done in preparation for direct anatomical reduction.
Anterolateral approach Retraction of the tibialis anterior muscle should be limited, to show only the essential part of the anterolateral surface of the tibia. Near the junction of the middle and lower thirds of the tibia, the anterior compartment vessels (Anterior Tibial) and nerve (Deep Peroneal) come together and approach the lateral tibial surface. They wrap obliquely anteriorly and distally around the tibia. In the distal metaphyseal area, they lie on the periosteum, under the myotendinous portion of tibialis anterior, extensor hallucis longus, and extensor digitorum longus. If this exposure extends into the distal third of the tibia, the surgeon should identify and protect the neurovascular bundle. With care, it can be mobilized from the tibial surface, along with the anterior compartment muscles. This makes it possible to pass a plate more distally on the anterolateral surface, all the way to the ankle joint, if necessary.
Posteromedial approach Skin incision The length of the incision varies according to fracture location and selected plate. The posteromedial boarder of the tibia is first palpated throughout its length. The incision is then made in parallel 1-2 cm posterior to the posterior tibial boarder. Dissection Subcutaneous dissection follows carefully so as to identify and/or protect the saphenous vein and nerve. These are typically mobilized anteriorly.
Posteromedial approach The fascia is then incised in line with the skin incision and the superficial and deep posterior compartments are mobilized. Gastrocnemius, soleus and flexor digitorum will be identified and mobilized with a soft-tissue elevator, depending on the level of the fracture. The dissection should be done in an extra-periosteal plane.Dissection is not necessary beyond the posterolateral aspect of the tibia.In this way, the middle 3/5 of the posterior tibia can be effectively exposed.
Posterolateral approach Skin incision The length of the incision varies, but it should begin over the lateral boarder of the gastrocnemius muscles and extend distally to a point that is midway between the achilles tendon and the fibula. The interval between the lateral and posterior compartments is usually easier to find distally. Further dissection proximally is undertaken as required.