Download
1 / 26
260 likes | 465 Views
Diffusion, partial pressures, and acid-base physiology. Lecture 13 Friday, February 9, 2007 Refs. Medical Physiology Chapters 25, 26 and 27, and Ganong. Factors in exchange of gasses. Diffusion over short distances Increase in thickness of alveolar septum decreases exchange

E N D
Diffusion, partial pressures, andacid-base physiology Lecture 13 Friday, February 9, 2007 Refs. Medical Physiology Chapters 25, 26 and 27, and Ganong
Factors in exchange of gasses • Diffusion over short distances • Increase in thickness of alveolar septum decreases exchange • Respiratory pigments • Hemoglobin greatly increases O2 uptake • Hemoglobin binds about 96% of O2 that diffuses into capillary. • Convection on both sides of barrier makes diffusion most efficient • Movement of air • Movement of blood
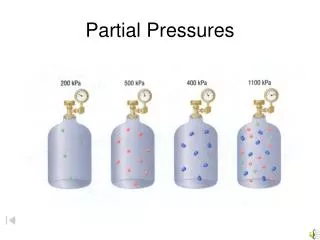
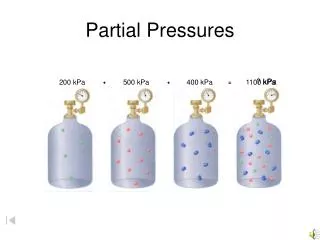
Composition of dry air • Gas Fraction (%) Partial Pressure • N2 78.09 593.48 • O2 20.95 159.22 • CO2 0.03 0.23 • Argon 0.93 7.07 • H2O 0 0 • Total 100 760
Dalton’s Law • Total pressure = sum of partial pressures of each gas • Partial pressure is mole fraction x total pressure • e.g. for O2 0.2095 x 760 = 159.22 mm Hg • When air is in contact with water, water vapor will be part of the gas mixture. • At 37°C partial pressure of water is 47 mm Hg. • To correct for water, P = (760-47) x dry fraction. • e.g. for O2 713 x 0.2095 = 149.37 mm Hg
Partial pressures of gasses • Gas Dry Air Wet air (trachea) • N2 593.48 556.78 • O2 159.22 149.37 • CO2 0.23 0.21 • Argon 7.07 6.63 • H2O 0 47 • Total 760 760
Diffusion of gas depends on: • Gradient • Simplified Fick’s Law: Flux is proportional to concentration difference and since concentration is proportional to partial pressure, flux is proportional to the difference in partial pressures. • Surface area • About 300 million alveoli in human lung • Combined area of 50 to 100 m2 • Solubility in aqueous • Henry’s Law: [C]Dis = s x PC (s is solubility). • For O2 at 37°, s = 0.0013 mM/mm Hg • For CO2 at 37°, s is about 23-fold higher (~.03)
Total cross sectional area is greatest in smallest airways. Velocity of air is inversely proportional to cross sectional area. MP 25-5
Acid-base physiology • H+ regulation is very important. • Cell processes are very sensitive to pH • Enzymes work best at their optimum pH • Changes in pH can open membrane channels • Changes in pH can activate or inhibit membrane transporters • Normal pH of plasma is 7.4 (H+ concentration = 0.00004) • Acidosis - pH < 7.4 • Alkalosis- pH > 7.4 • Range compatible with life is 7.00 to 7.7
H+ Balance • H+ load is generated by metabolism. • Gluconeogenesis in liver (fig. 39-3) produces urea, glutamine, and phosphate and sulfate anions. • Enzymes in the kidney convert glutamine to ammonium and HCO3- • Exercise increases H+ load • CO2 formed in tissues becomes H2CO3
Buffering • The general equation for a buffer system is the Henderson-Hasselbalch Equation. • The buffering capacity of a system is greatest when the amount of free anion is equal to the amount of undissociated acid. • Most effective buffering occurs when pH = pK • In biological systems it is apparent pK.
Buffering • The general equation for a buffer system is the Henderson-Hasselbalch Equation. • The buffering capacity of a system is greatest when the amount of free anion is equal to the amount of undissociated acid. • Most effective buffering occurs when pH = pK • In biological systems it is apparent pK.
3 buffering systems in blood • Plasma proteins • Free carboxyl and free amino groups dissociate • Hemoglobin (histidine residues) • Each hemoglobin molecule has 38 histidine residues • 6 times the buffering capacity of the plasma proteins • Carbonic acid-bicarbonate
Buffering by bicarbonate The pK is only about 3, but carbonic acid is in equilibrium with CO2.
The bicarbonate system is an effective buffer even though the the pK is low because the amount of CO2 is controlled by respiration Ganong
Bicarbonate buffering • Plasma concentration of HCO3- is regulated by the kidneys. • When H+ is added HCO3- decreases as H2CO3 is formed. • H2CO3 is converted to CO2 and H2O and the CO2 is excreted by the lungs. • Increased H+ stimulates respiration and produces a drop on PCO2
Respiratory acidosis/alkalosis • Respiratory acidosis- a decrease in ventilation causes a rise in PCO2 • Renal compensation • Increased renal tubular secretion of H+ • Increased resorption of HCO3- from filtrate • Respiratory alkalosis- a decline in PCO2 • Renal compensation • Low PCO2 decreases renal H+ secretion and resorption of HCO3
Metabolic acidosis/alkalosis • Metabolic acidosis- when acid stronger than HHb is added to blood. • Renal compensation - increased renal H+ excretion • Respiratory compensation-increases in H+ stimulates respiration • Metabolic alkalosis- when H+ level falls after addition of alkali or removal of acid • Respiratory compensation is a decrease in respiratory rate.