Download
1 / 22
240 likes | 486 Views
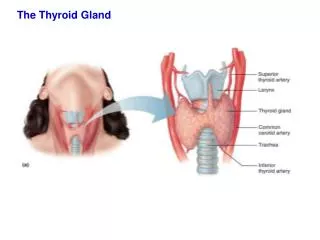
The Thyroid Incidentaloma. Dimyati Achmad Department of Surgery Faculty of Medicine Padjadjaran University/ Hasan Sadikin Hospital Bandung Indonesia.

E N D
The Thyroid Incidentaloma DimyatiAchmad Department of Surgery Faculty of Medicine Padjadjaran University/ HasanSadikin Hospital Bandung Indonesia
Female, 70 years old after cancer resection 6 months ago due to anal cancer, undergo positron emission tomography to determine distant metastases. • There is no sign and symptom thyroid gland disorder on physical examination. • PET Exam. revealed: No sign of distant metastases, but there is a focal uptake in the thyroid gland.
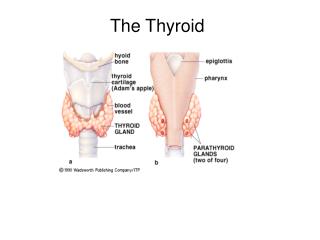
Introduction Thyroid Incidentaloma (T.I.) Is a thyroid lesions detected during Imaging investigation unrelated to examination of thyroid gland
Prevalency of T.I. increased as the extent of use Ultrasonography (USG), Computed Tomography (CT), Magnetic Resonance Imaging (MRI) and especially Positron Emission Tomography (PET).
CurrentlyPET scans with 18F flourodeoxyglucose(FDG-PET) are widely used in the management of patients with malignant conditions of various organ systems, especially to determine the extent of the primary tumor, regional nodal metastases and distant metastases.
Until today the management of T.I. is still dilemmatic whether put on further investigationor not.
This problems has actually been there before but again brought attention due to development imaging technology such as PET scans.
We review some articles about T.I. to conclude the appropriate management.
There are some clinical features of T.I. suspicious malignant Gender : Male Age : < 20 years or > 60 years Prior head and neck irradiation Family history of thyroid carcinoma Lateral neck lymphadenophaty
USG Examination Prevalence of T.I. : 9,4 % - 27 % Characteristics of suspicious malignant : 1. Microcalcification 2. Irreguler margin 3. Incomplete halo.
CT / MRI Examination Prevalence of T.I. : CT : + 11.3% MRI : + 13% CT or MRI examination can not be revealed the malignant form because there is no characteristic to differentiated them.
PET Examination Prevalence of T.I. : 1.1% - 8.4% Mostly of cases are benign lesions. 32.4% malignant cases : the most histopatology result is micropapillary thyroid carcinoma which is a slow growing, good prognosis and the 10-year diseases specific mortality < 1%
FDG uptake in the thyroid gland, PET interpretation which was greater than background activity in adjacent tissues and blood pool, was classifed as : Focal Multifocal Diffuse Focal uptake descriptionindicated is neoplastic process.
PET Interpretation Standart Uptake Value (SUV) The relationship betweenmalignant with SUV is still debatable. Size of nodule No significant different between nodule > 1 cm in diameter compared with 1 cm or lessnodule in diameter to determine malignancy.
The Principles of T.I. Management • We should be considered the balancing between benefitof early diagnosis and treatment with cost-effectiveness. • The prognosis of the primary tumorshould be take into account before investigating a potential thyroid lesion.
There is no benefit to investigate T.I. in patient with widespread distant metastasis and poor overall survival from the primary tumor.
we summarized the management of T.I. in an algorithm, hopefullycan explain the related dilematic issues. We emphasized in yellow highlight form.
PET. Exam Focal Multifocal / Diffuse Management Algorithm for T.I. CT/MRI Clinical Feature Suspicious Malignancy Non Suspicious Malignancy USG Exam Suspicious Malignancy Non Suspicious Malignancy Regular Follow - up with USG USG-Guided FNA Malignant or Suspicious Benign Surgery
Conclusions • Until today, the management of T.I. is still controversial. • We should be considered the balancing between benefitof early diagnosis and treatment with cost-effectiveness
In cases of T.I. which are male, age < 20 years or > 60 years, previous head and neck irradiation, family history of thyroid cancer and lateral neck lymphadenopathy which should be undergo further investigation. • In case without clinical features of malignancy we can do observation with repeat ultrasound to evaluate change of size and determine sign malignancy based on USG characteristics.