Download
1 / 24
280 likes | 787 Views
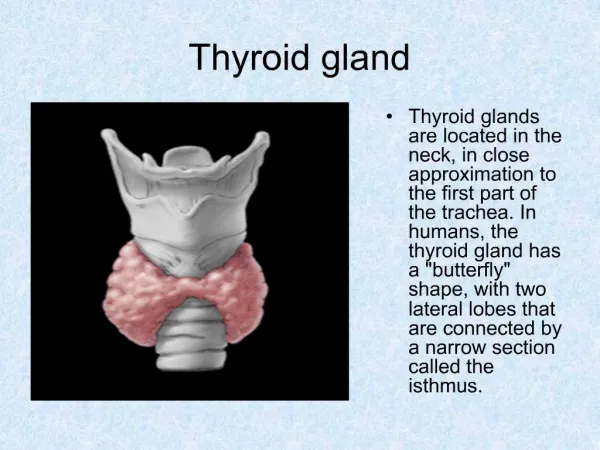
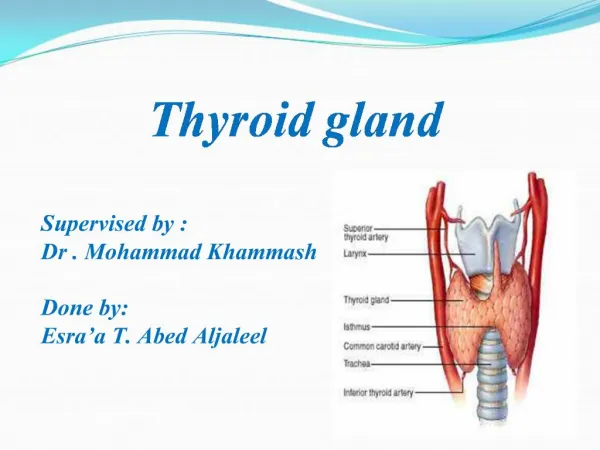
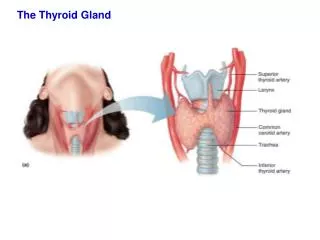
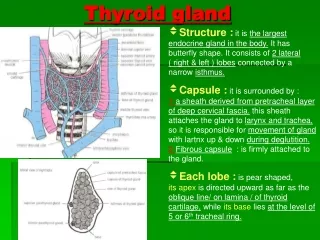
THE THYROID GLAND. Anatomy, Histology, Physiology. Situated in the anterior neck Macroscopic : two lobes connected through the isthmus Microscopic :- follicles which contain the colloid and are surrounded by a single layer of thyroid epithelium

E N D
Anatomy, Histology, Physiology • Situated in the anterior neck • Macroscopic : two lobes connected through the isthmus • Microscopic :-follicles which contain the colloid and are surrounded by a single layer of thyroid epithelium The follicle cells synthesize thyroglobulin (Tg) which is extruded into the lumen of the follicle. The biosynthesis of T4, T3 occurs within Tg at the cell-coloid interface.( Tg =large GP containing 140 tyrosyl residues) ! Sufficient iodide is necessary to allow the synthesis of TH Thyroidal peroxidaze (TPO) is a membrane-bound GP, available at the cell coloid interface for iodination and hormonogenesis in Tg. Thyroid hormone synthesis and secretion • Involves several major steps: 1) active transport of I- across the BM into the thyroid cell (trapping of iodide)→ by an intrinsec membrane protein =Na+/I- symporter (NIS) • The NIS is ●( +) by TSH and TSH rec- stimulating antibody (TRAb) found in Grave’ s disease ●saturable with large amounts of iodide ● (-) by ions such as ClO4-( perchlorate), TcO4- (pertechnetatea)
Physiology 2)oxidation of iodide:I- I2 and iodination of thyrosyl residues in Tg to form iodothyrosine (MIT, DIT) [ =I organification] ← catalyzed by TPO 3)coupling of iodotyrosine molecules within Tg to form iodothyronines (T3,T4) ← also mediated by TPO MIT+DIT=T3 DIT+DIT=T4 !!! Thiocarbamide drugs- particularly propylthiouracil, methimazole, carbimazole- are potent inhibitors of TPO and will block thyroid hormone synthesis. 4) proteolysis of Tg, with release of free iodothyronines and iodotyrosines ( at the cell-colloid interface, colloid is engulfed into a colloid vesicle and is absorbed into the thyroid cell → the lysosomes then fuse with the colloid vesicle and hydrolysis of Tg occurs, releasing T4, T3, DIT, MIT; T4, T3 are released into circulation THYROID HORMONE TRANSPORT TH are transported in serum bound to carrier protein :TBG, TBPA, Albumin Although only 0,04% of T4 and 0,4% of T3 are “free”, it is the free fraction that is responsible for hormonal activity !!! The levels of free H are normal in states where there are primary or secondary changes in plasma binding proteins, because TSH release is controlled by the free thyroid hormone level and adjusts to normalize it irrespectively of how much hormone is bound by the plasma proteins. ! The active form in peripheral tissues is T3 Most of the plasma pool of T3 is derived from peripheral metabolism (5’-deiodination ) of T4
Thyroid hormones biosynthesis • Iodide transport (the iodide trap) • Iodination of thyrosil in thyroglobulin →MIT, DIT • Coupling of iodotyrosyl residues in thyroglobulin→ • T3, T4 Apical microvilli Basement membrane Na- Colloid Tyr I- TPO I- Tg Na/I symporter TBG-carrier protein of TH Tissue monodeiodinaze
Goiter= enlargement of the thyroid gland • Nontoxic goiter (ie, goiter not associated with hyperthyroidism) can be diffuse or nodular. Criteria –clinic : 4 grades in OMS classification Grade 1= small goiter; it can’t be observed with the head in a normal position( only with the head in hyperextension), but it can be palpated Grade 2=moderate goiter; physical examination: visible with the head in normal position, palpable; it does not extend beyond the external branch of sternocleidomastoid muscle Grade 3=large goiter: one or both lobes extend beyond the external branch of sternocleidomastoid muscle; it is visible from 10 m distance; ± pressure symptoms in the neck Grade 4= huge goiter; extend inferiorly to present as substernal goiter and superiorly towards the mandible; it totally deforms the neck and it can be “seen” from behind ; it is accompanied by important pressure symptoms in the neck
Etiology of nontoxic goiter: Iodine deficiency Hashimoto’s thyroiditis Subacute thyroiditis Inadequate hormone synthesis due to inherited defect in thyroidal enzymes necessary for T4,T3 biosynthesis Neoplasm, benign or malignant • Criteria- ultrasonographic: goiter volume The upper normal limits in Women=16 ml Men=18ml ! In some cases, nontoxic goiter results from TSH stimulation, which in turn results from inadequate TH synthesis. Some goiters ← to mutations in genes involved in thyroid growth and/or thyroid function. In many patients, however, the cause of the goiter is obscure, because serum TSH levels are normal
ENDEMIC GOITER • Worldwide, iodine deficiency remains the most common cause of nontoxic goiter or endemic goiter • Definition: any goiter occurring in a region where goiter is prevalent (>10% of children in the population have a thyroid enlargement) • Optimal iodine requirements for adults:100-150 g/day (200-300g/zi)( during pregnancy and lactation: 200 g/day ) In endemic goiter areas the daily intake (and urinary excretion) of iodine falls <50 g/day→ the gland is unable to maintain adequate hormonal secretion, and thyroid hypertrophy ( goiter) and hypothyroidism result. PATHOGENESIS : The development of nontoxic goiter in patients with severe iodine deficiency ( or with dyshormonogenesis) involves impaired TH synthesis and, secondarily, ↑ in TSH secretion, → diffuse thyroid hyperplasia ± focal or nodular hyperplasia → over an extended period of time a diffuse, nontoxic goiter may progress → to multinodular nontoxic goiter → toxic multinodular goiter (with hyperthyroidism) ! The mechanism for the development of autonomous growth and function of thyroid nodules may involve some activating mutations (Gs protein in the cell membrane) which result in thyroid cell proliferation and hyperfunction even when TSH is suppressed.
ENDEMIC CRETINISM • Severe hypothyroidism in infancy is termed cretinism. Retardation of mental development and growth are the hallmark of cretinism. • Endemic cretinism is a development disorder that occurs in regions of severe endemic goiter. Both parents of an endemic cretin are usually goitrous. And in addition to the features of sporadic cretinism, endemic cretins often have deaf-mutism, spasticity, motor dysfunction, and abnormalities in the basal gnglia. • 3 types of cretins can be discerned : • Hypothyroid cretins • Neurologic cretins • Cretins with combined features of two
CLINICAL PICTURES • thyroid enlargement diffuse or multinodular • neck dicomfort • Pressure symptoms: large, huge goiter which may displace or compress adjacent structures such as trachea, esophagus, neck vessels → dyspnea, inspiratory stridor, dysphagia, chocking sensation, facial flushing and dilatation of cervical veins on lifting the arms over the head • compression of the recurrent laryngeal nerve, with hoarseness- rare • usually not associated with abnormal thyroid hormone secretion, but endogenous subclinical thyrotoxicosis caused by autonomously nodules may develop ; rarely hypothyroidism PHYSICAL EXAMINATION goiter size→ OMS classification consistency: may be relatively firm, but it is often soft or rubbery shape, structure : diffuse (smooth) or nodular mobility with deglutition and sub adjacent structures tenderness the presence of latero- cervical adenopathy
Laboratory findings • 1. THYROID ULTRASONOGRAPHY : assesses both morphology and the size of the goiter; useful for measuring the size of individual nodules and for evaluating the results of therapy; for differentiating solid from cystic lesion; is a simple way to follow the growth of the goiter and nodules ; also used to guide the operator to a deep nodule during FNAB • 2. SCINTIGRAPHY (ISOTOPE SCANNING) → a patchy uptake, frequently with focal areas of increased uptake corresponding to “hot” nodules and areas of ↓ uptake → “cold” nodule ( !!!10% of surgically removed cold nodule=malignant) • 3. RAIU– values N/( high iodine uptake- in endemic regions) ( =I avidity, not hyperthyroidism !!!/↓ depending on the iodide pool and TSH levels • 4. HORMONAL DETERMINATIONS : TSH, FT4 –usually normal • 5. THYROID AUTOANTIBODIES : TPO Ab, Tg Ab- high titers in autoimmune thyroid disease • 5. CONVENTIONAL RADIOGRAPHY OF THE NECK AND THE UPPER MEDIASTINUM → tracheal compression
Laboratory findings • 6. NECK AND MEDIASTINAL CT/ MRI → in the presence of intrathoracic goiter to define the relationship with surrounding structures • 7. LARINGOSCOPHY – vocal cord paralysis • 8. FNAB of a thyroid nodule→ in malignity suspicion; it has been proved to be the best method for differentiation of benign from malignant thyroid disease; it may have therapeutically utility → draining a cyst
Treatment • A. MEDICAL TREATEMENT :in diffuse goiter and multinodular goiter ( after excluding malignity) a. IODIDE → diffuse goiter, youth • KI 1 mg 2tb/week • JODID 100-200 g/day b. L-T4 25-50 g/day → nontoxic multinodular goiter (= suppressive therapy) c. I+L-T4 • JODTHYROX (100 g I+ 100 g L-T4) /tb ½ tb/day d. Treating the hyperthyroidism when a multinodular goiter becomes toxic with one or more hyperfunctional nodules/ hypothyroidism
Treatment • B. SURGICAL TREATMENT • For goiter that continues to grow despite TSH suppression with LT4 • for goiters that produce obstructive symptoms, with substernal extension C. PROPHYLAXI IODIDE for risk groups : pregnancy, lactation, ages: 6-14 and 14-18
THYROIDITIS CLASSIFICATIONCLASIFICAREA TIROIDITELOR • 1. ACUTE thyroiditis • 2. SUBACUTE thyroiditis • 3. CHRONIC thyroiditis • Autoimmune • Fibrous
ACUTE THYROIDITIS (THYROID ABSCESS ) • =acute bacterial inflammation of thyroid gland which untreated → abscess • Etiology: staphilococ, streptococ, germeni gram negative bacteria, fungi • rare; may appear in the context of septicemia or acute infective endocarditis • Acute onset • Clinic • GENERAL signs : malaise, fever, sweating • LOCAL signs : pain and tenderness, swelling and warmth and redness of the underlying skin • Satellite adenopathy
LABORATORY FINDINGS • ↑↑ ESR • FBC- anemia, ↑ neutrophyls • Thyroid scintigraphy : no uptake corresponding to the affected thyroid area • Thyroid ultrasonography : → the abscess or evidence of swelling • Needle aspiration will confirm the diagnosis and identify the organism TREATMENT • ANTIBIOTIC THEARPY ± occasionally EXCISION/ DRAINAGE (ABSCESS)
SUBACUTE THYROIDITIS (DE QUERVAIN’ S THYROIDITIS) • or granulomatous thyroiditis; = an acute inflammatory disorder of the thyroid gland most likely due to viral infection : mumps, adenoviruses… • CLINIC • Subacute onset ; usually- !an episode of upper respiratory tract infection in the previous weeks • Pain, soreness in the neck, which may extend up to the angle of jaw or toward the ear lobes on one or both sides of the neck • Thyroid enlargement • Initially, the patient may have symptoms of hyperthyroidism: palpitation, agitation, sweats • General signs: fever, malaise
LABORATORY FINDINGS • ↑ ESR (sometimes =100mm/h) • Initially :↑ T3,T4 + ↓TSH + ↓↓ RAIU; as the disease progress –T3,T4 will ↓ and TSH will ↑( and symptoms of hypothyroidism are noted ); later RAIU ↑ (→ recovery of the gland from the acute insult) • Thyroid scinthygraphy - no uptake “white” • Thyroid ultrasonography –hypoechogene aspect corresponding to the affected area • TREATMENT • Prednisone 50-60 mg/day, decreasing progressively the dosage • -blocker • sedative • L-thyroxine – during the hypothyroid phase
CHRONIC THYROIDITIS (HASHIMOTO’S THYROIDITIS, LYMPHOCYTIC THYROIDITIS ) • an immunological disorder in which lymphocytes become sensitized to thyroidal antigens and autoantibodies are formed that react with these antigens Pathology : heavy infiltration of lymphocites totally destroiyng normal thyroidal architecture • CLINIC • Firm goiter /small, atrophic thyroid gland • Euthyroid / mild hypothyroidism →severe • rarely- “HASHITOXICOSIS ”→ may go through periods of activity when large amounts of T3,T4 are released or “ dumped”, resulting in transient symptoms of thyrotoxicosis ( =“spontaneously resolving hyperthyroidism ) ! One variant of Hashimoto’s thyroiditis has been termed “silent” or “painless” thyroiditis (→ predilection: the postpartum period) ; evolves with a triphasic course, similar to what is seen in subacute thyroiditis : mild hyperthyroidism (1-3 months)→ hypothyroid phase (several months) →recovery ! Reccurent episodes
CHRONIC THYROIDITIS (HASHIMOTO’S THYROIDITIS) • COMPLICATIONS: progressive hypothyroidism • COURSE : may develop other autoimmune diseases: pernicious anemia, adrenal insufficiency, DM type1 • LABORATORY FINDINGS • ESR=normal • TSH, T3, T4 vary with the course of disease; usually normal/ ↑ TSH ± ↓ T3,T4 / ↓ TSH, ↑T3,T4 • Thyroid ultrasonography: diffuse hypoechogene aspect ← Ly infiltrate • TPO Abs , Tg Abs =the most striking laboratory findings TREATMENT • Replacement treatment with LT4 – overt hypothyroidism • B-blocker –hyperthyroid phase of silent or postpartum thyroiditis
RIEDEL’ THYROIDITIS • rare • → characterized by fibrosis of the thyroid gland and adjacent structure • CLINIC • insidious onset • goiter –usually as stony-hard mass with extensive fibrosis extending outside the gland and involving overlying muscle and surrounding tissue • compression signs of adjacent structure : TRACHEA, ESOPHAGUS and LARYNGEAL NERVES • Euthyroid /mild hypothyroidism • surgery may be required to preserve tracheal and esophageal function • ! Must be differentiated from thyroid cancer