Download
1 / 1
20 likes | 214 Views
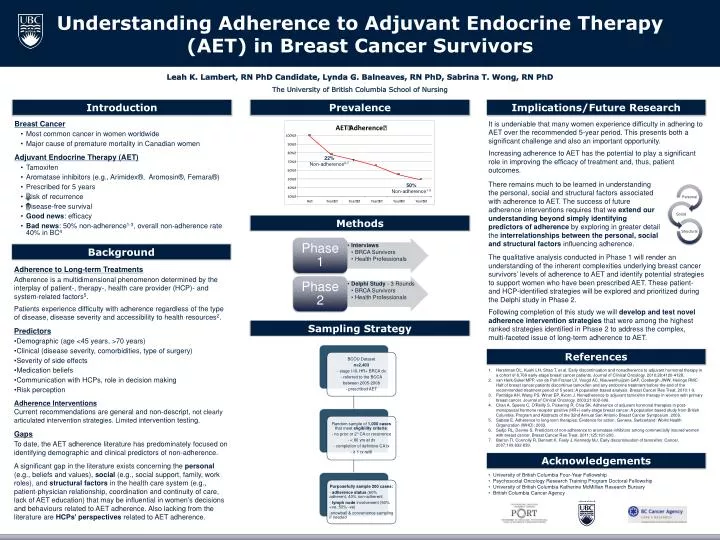
Introd uction. Prevalence. Implications/Future Research. It is undeniable that many women experience difficulty in adhering to AET over the recommended 5-year period. This presents both a significant challenge and also an important opportunity.

E N D
Introduction Prevalence Implications/Future Research It is undeniable that many women experience difficulty in adhering to AET over the recommended 5-year period. This presents both a significant challenge and also an important opportunity. Increasing adherence to AET has the potential to play a significant role in improving the efficacy of treatment and, thus, patient outcomes. Breast Cancer • Most common cancer in women worldwide • Major cause of premature mortality in Canadian women Adjuvant Endocrine Therapy (AET) • Tamoxifen • Aromatase inhibitors (e.g., Arimidex®, Aromosin®, Femara®) • Prescribed for 5 years • Risk of recurrence • Disease-free survival • Good news: efficacy • Bad news: 50% non-adherence1-3, overall non-adherence rate 40% in BC4 22% Non-adherence6-7 There remains much to be learned in understanding the personal, social and structural factors associated with adherence to AET. The success of future adherence interventions requires that we extend our understanding beyond simply identifying predictors of adherence by exploring in greater detail the interrelationships between the personal, social and structural factors influencing adherence. 50% Non-adherence1-3 Methods Background The qualitative analysis conducted in Phase 1 will render an understanding of the inherent complexities underlying breast cancer survivors’ levels of adherence to AET and identify potential strategies to support women who have been prescribed AET. These patient- and HCP-identified strategies will be explored and prioritized during the Delphi study in Phase 2. Following completion of this study we will develop and testnovel adherence intervention strategies that were among the highest ranked strategies identified in Phase 2 to address the complex, multi-faceted issue of long-term adherence to AET. Adherence to Long-term Treatments Adherence is a multidimensional phenomenon determined by the interplay of patient-, therapy-, health care provider (HCP)- and system-related factors5. Patients experience difficulty with adherence regardless of the type of disease, disease severity and accessibility to health resources2. Predictors • Demographic (age <45 years, >70 years) • Clinical (disease severity, comorbidities, type of surgery) • Severity of side effects • Medication beliefs • Communication with HCPs, role in decision making • Risk perception Adherence Interventions Current recommendations are general and non-descript, not clearly articulated intervention strategies. Limited intervention testing. Gaps To date, the AET adherence literature has predominately focused on identifying demographic and clinical predictors of non-adherence. A significant gap in the literature exists concerning the personal (e.g., beliefs and values), social (e.g., social support, family, work roles), and structural factors in the health care system (e.g., patient-physician relationship, coordination and continuity of care, lack of AET education) that may be influential in women’s decisions and behaviours related to AET adherence. Also lacking from the literature are HCPs’ perspectives related to AET adherence. Sampling Strategy References Hershman DL, Kushi LH, Shao T, et al. Early discontinuation and nonadherence to adjuvant hormonal therapy in a cohort of 8,769 early-stage breast cancer patients. Journal of Clinical Oncology. 2010;28:4120-4128. van Herk-Sukel MPP, van de Poll-Franse LV, Voogd AC, Nieuwenhuijzen GAP, Coebergh JWW, Herings RMC. Half of breast cancer patients discontinue tamoxifen and any endocrine treatment before the end of the recommended treatment period of 5 years: A population-based analysis. Breast Cancer Res Treat. 2010:1-9. Partridge AH, Wang PS, Winer EP, Avorn J. Nonadherence to adjuvant tamoxifen therapy in women with primary breast cancer. Journal of Clinical Oncology. 2003;21:602-606. Chan A, Speers C, O'Reilly S, Pickering R, Chia SK. Adherence of adjuvant hormonal therapies in post-menopausal hormone receptor positive (HR+) early-stage breast cancer: A population based study from British Columbia. Program and Abstracts of the 32nd Annual San Antonio Breast Cancer Symposium. 2009. Sabate E. Adherence to long-term therapies: Evidence for action. Geneva, Switzerland: World Health Organization (WHO); 2003. Sedjo RL, Devine S. Predictors of non-adherence to aromatase inhibitors among commercially insured women with breast cancer. Breast Cancer Res Treat. 2011;125:191-200. Barron TI, Connolly R, Bennett K, Feely J, Kennedy MJ. Early discontinuation of tamoxifen. Cancer. 2007;109:832-839. Acknowledgements • University of British Columbia Four-Year Fellowship • Psychosocial Oncology Research Training Program Doctoral Fellowship • University of British Columbia Katherine McMillian Research Bursary • British Columbia Cancer Agency