Download
1 / 26
300 likes | 861 Views
Blood and Tissue Protozoa. Mark F. Wiser Department of Tropical Medicine School of Public Health. Protozoa of Blood and Tissues. Disease Causing Kinetoplastids. African trypanosomes sleeping sickness Trypanosoma cruzi Chagas’ disease S. and Central America Leishmania species

E N D
Blood and Tissue Protozoa Mark F. Wiser Department of Tropical Medicine School of Public Health
Disease Causing Kinetoplastids • African trypanosomes • sleeping sickness • Trypanosoma cruzi • Chagas’ disease • S. and Central America • Leishmania species • leishmaniasis • focal distribution worldwide Kinetoplast Nucleus KT = mitochondrial DNA
Disease Course and Symptoms • invasion of blood characterized by irregular fever and headache (acute stage) • T. gambiense can be self-limiting or progressing to a more serious disease (chronic) • includes invasion of lymphatics and CNS • parasites crossing blood-brain barrier result in CNS involvement and nervous impairment • described as meningoencephalitis • increased apathy and fatigue • confusion and somnolence • motor changes including tics, slurred speech, incoordination • convulsions, coma, death
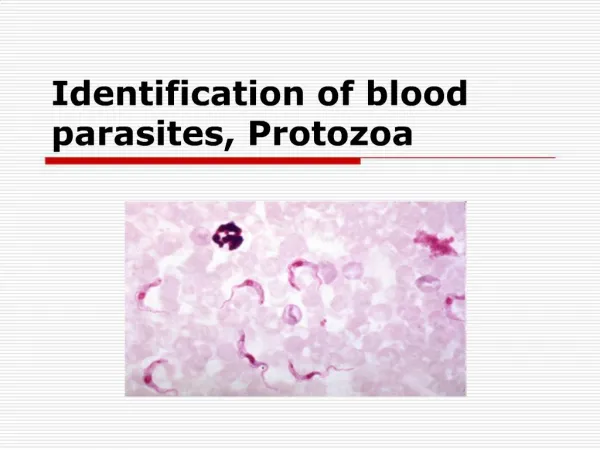
Diagnosis and Treatment • Clinical Features • travel or residence in endemic area • irregular fever and enlarged lymph nodes • behavioral changes/mental symptoms • Laboratory Diagnosis • serological tests • demonstration of trypanosomes in blood, lymph node aspirates, cerebral spinal fluid • Early Stage • No CNS involvement • suramin • pentamidine • excellent prognosis • Late Stage • CNS involvement • melarsoprol • eflornithine (resurrection drug)
Trypanosoma cruziand Chagas Disease • Transmitted by triatomine bugs • Inefficient transmission (parasite in feces of bug) • Associated with infestation of houses with triatomines (rural poverty) • Urban transmission associated with blood transfusions • Leading cause of cardiac disease in S. and central America
Clinical Course of Chagas • Acute Phase • active infection (1-4 months) • most are asymptomatic (children most likely to be symptomatic) • Indeterminate Phase • 10-30 years of latency • seropositive with no detectable parasitemia • Chronic Phase • 10-30% of infected exhibit cardiomyopathy • arrhythmias and conduction defects • congestive heart failure • thromboembolic phenomenon
Leishmaniasis • focal distribution throughout world, especially tropics and subtropics • new world: southern Texas to northern Argentina • old world: Asia, Africa, middle east, Mediterranean • transmitted by sand flies • new world: Lutzomyia • old world: Phlebotomus • parasite replicates within macrophages of vertebrate host • a variety of disease manifestations
Clinical Spectrum of Leishmaniasis • Cutaneous Leishmaniasis (CL) • most common form, relatively benign self-healing skin lesions (aka, localized or simple CL) • Mucocutaneous Leishmaniasis (MCL) • simple skin lesions that metastasize to mucosae (especially nose and mouth region) • Visceral Leishmaniasis (VL) • generalized infection of the reticuloendothelial system, high mortality
Diagnosis • geographical presence of parasite • demonstration of parasite in skin lesion or bone marrow • delayed hypersensitivity skin test (cutaneous forms) • serological tests (visceral disease) Treatment • pentavalent antimonials • amphotericin B (less toxic, expensive) • miltefosine (phase IV, no hospitalization)
MALARIA • causative agent = Plasmodium species • 4 human Plasmodium species • 40% of the world’s population lives in endemic areas • primarily tropical and sub-tropical • 3-500 million clinical cases per year • 1.5-2.7 million deaths (90% Africa) • increasing problem (re-emerging disease) • resurgence in some areas • drug resistance ( mortality) P. falciparum P. vivax P. ovale P. malariae
Life Cycle • transmitted by Anopheles mosquitoes • sporozoites injected with saliva • sporozoites invade liver cells • undergo an asexual replication • 1000-10,000 merozoites produced • hypnozoites and relapses in Pv and Po
Life Cycle • merozoites invade RBCs • repeated rounds of asexual replication • 6-30 merozoites formed
Life Cycle • some merozoites produce gametocytes • gametocytes infective for mosquito • fusion of gametes in gut • sporogony on outside of gut wall • asexual replication • sporozoites invade salivary glands
Clinical Features • due to the blood stage of the infection • no symptoms during liver stage (~ incubation period) • characterized by acute febrile attacks (malaria paroxysms) • periodic episodes of fever alternating with symptom-free periods • manifestations and severity depend on species and host status • acquired immunity • general health • nutritional state • genetics
Malaria Paroxysm • paroxysms associated with synchrony of merozoite release • 48 or 72 hr cycles • release of antigens, etc • TNF- • temperature is normal and patient feels well between paroxysms • falciparum may not exhibit classic paroxysms • continuous fever • paroxysms become less severe and irregular as infection progresses
P. falciparum expresses ‘knobs’ on the surface of infected erythrocytes. Knobs mediate cytoadherence to endothelial cells.
Falciparum Complications • sequestration of Pf-infected erythrocytes • immune evasion • primarily in brain, heart, lungs, and gut • leads to complications • cerebral malaria • consciousness ranges from stupor to coma • convulsions frequently observed • onset can be gradual or sudden • mortality 30-50%
Possible Pathophysiology cytoadherence cerebral ischemia hypoxia, metabolic effects, cytokines (eg, TNF-) coma death
Severe falciparum malaria • potentially high parasitemias • sequestration • complex (and not fully understood) host-parasite interactions
Malaria Diagnosis • symptoms: fever, chills, headache, malaise, etc. • history of being in endemic area • splenomegaly and anemia as disease progresses • microscopic demonstration of parasite in blood smear (distinguish species) • thick film: more sensitive • thin film: species identification easier • repeat smears every 12 hours for 48 hours if negative • antigen detection ‘dipstick’ • ParaSight-F, OptiMal, etc
Treatment Strategies • chloroquine sensitive (all species) • chloroquine • CQ + primaquine (vivax/ovale) • chloroquine resistance (or unknown) • Fansidar, mefloquine, quinine, artemisinin derivatives • severe malaria • i.v. infusion of quinine or quinidine (or CQ, if sensitive) • i.v. artemisinin derivatives (if available)