Download
1 / 47
470 likes | 663 Views
Administrative Principles of Vaccination Prof. Dr. AHMET ARVAS I.U. Cerrahpasa Medical Faculty , Department of Pediatrics. Vaccine preventable diseases. infant mortality in world -2010. Lancet 2012;380:2095-125. child mortality -2010 (1-4 y). Lancet 2012;380:2095-125.

E N D
AdministrativePrinciples of Vaccination Prof. Dr. AHMET ARVAS I.U. CerrahpasaMedicalFaculty, Department of Pediatrics
infantmortality in world-2010 Lancet 2012;380:2095-125
childmortality-2010 (1-4 y) Lancet 2012;380:2095-125
Vaccinepreventabledeaths in world-2008 Measles118.000 Hibinf.199.000 Pertussis195.000 Tetanus 2.000 N. Tetanus59.000 Yellowfever30.000 Diphteria4.000 Rotavirusinf.453.000 Pneumococcaldis.476.000 Hepatitis B inf. 10.000 1.5 million of deathsamongchildrenunder 5 yearsaredueto diseasesthatcouldhavebeenpreventedbyroutinevaccination
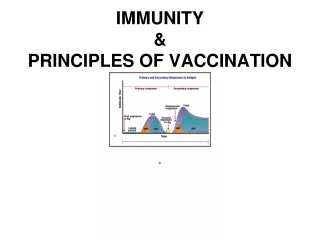
Activevaccination • Protectionproducedbyvaccine • Usuallypermanent • Immunityandimmunologicmemorysimilartonaturalinfection but without risk of disease
Classification of vaccines • Liveattenuated • bacterial • viral • Inactivated • whole: viruses, bacteria • fractional: protein based (toxoid, subunit) • polysaccharide-based (pure, conjugate)
Live Attenuated Vaccines • Attenuated (weakened) form of the "wild" virus or bacterium • Must replicate to be effective • Immune response similar to natural infection • Usually produce immunity with one dose (exceptthoseadministratedorally) *except those administered orally
Inactivated Vaccines • Cannot replicate • Generally not as effective as live vaccines • Less interference from circulating antibody than live vaccines • Generally require 3-5 doses • Immune response mostly humoral • Antibody titer may diminish with time
General Rules • Inactivated vaccines are generally not affected by circulating antibody to the antigen • Live attenuated vaccines may be affected by circulating antibody to the antigen
Polysaccharide Vaccines Purepolysaccharide • pneumococcal • meningococcal • SalmonellaTyphi (Vi) • Haemophilusinfluenzae type b • Pneumococcal (PCV-7, PCV-10, PCV13) • Meningococcal (MenC, MCV4) Conjugate polysaccharide
2012 Immunization Schedule-Turkey birth 1 month 2 months 4 months 6 months Firstschoolgrade (6 yrs) Eighthschoolgrade (13-14 yrs) m m P v B PCV B MMR B OPV DaPT/IPV + HepA II Varicella ı
Immunizationcoverage rate in Turkey (%) Source: TurhishHealthMinistryPublicHealthInstitute
All vaccines can be administered at the same visit as all other vaccines
Spacing of Vaccine Combinations Not Given Simultaneously Minimum Interval 4 weeks None Combination twolive injected or intranasal influenza vaccine allother
Increasing the interval between doses of a multidose vaccine does not diminish the effectiveness of the vaccine. It is not necessary to restart the series or add doses because of an extended interval between doses • Decreasing the interval between doses of a multidose vaccine may interfere with antibody response and protection • Vaccine doses should not be administered at intervals less than the minimum intervals or earlier than the minimum age *after the series has been completed
Time limitsforusingvaccinesafterreconstitution MMR≤ 8 hrs BCG ≤ 4-8 hrsprotectfromligth Varicella ≤ 30 min
Types of administrationerrors • wrongvaccineorwrongdiluent • wrongedosage • expiredvaccine • wrongroute/site/needle size • wrong time • wrongpatient
Vaccine Adverse Reactions • Local • pain, swelling, redness at site of injection • common with inactivated vaccines • usually mild and self-limited
Vaccine Adverse Reactions • Systemic • fever, malaise, headache • nonspecific • may be unrelated to vaccine
Vaccine Adverse Reactions • Allergic • due to vaccine or vaccine component • rare • risk minimized by screening
Contraindication • A condition in a recipient that greatly increases the chance of a serious adverse reaction
Precaution • A condition in a recipient that might increase the chance or severity of an adverse reaction, or • Might compromise the ability of the vaccine to produce immunity
Contraindications Permanent contraindications to vaccination: • severe allergic reaction to a vaccine component or following a prior dose (anaphylacticreaction: allvaccines) • Encephalopathy/encephalitisnot due to another identifiable cause occurring within 7 days of pertussisvaccination • Severe combinedimmunodeficiency (livevaccines)
Immunosuppression • Disease • congenital immunodeficiency • leukemia or lymphoma • generalized malignancy • Chemotherapy • alkylating agents • antimetabolites • radiation
Immunosuppression • Corticosteroids • 20 mg or more per dayof prednisone* • 2 mg/kg or more per day of prednisone* • NOT aerosols, alternate day, short courses, topical *for 14 days or longer
Vaccination of householdcontactsof immunosuppressedpersons • Healthy household contacts of immunosuppressed persons should receive MMR and varicella vaccines and annual influenza vaccination
Invalid contraindicationsto vaccination • Mild illness • Antimicrobial therapy • Disease exposure or convalescence • Pregnant or immunosuppressed person in the household • Breastfeeding • Preterm birth • Allergy to products not present in vaccine or allergy that is not anaphylactic • Family history of adverse events • Tuberculin skin testing • Multiple vaccines
Vaccination duringacute illness • No evidence that acute illness reduces vaccine efficacy or increases vaccine adverse reactions • Vaccines should be delayed until the illness has improved • Mild illness, such as otitis media or an upper respiratory infection, is NOT a contraindication to vaccination
Missed opportunity A healthcare encounter in which a person is eligible to receive vaccination but is not vaccinated completely
Reasons for missedopportunities • Lack of simultaneous administration • Unaware child needs additional vaccines • Invalid contraindications • Inappropriate clinic policies
Vaccine Adverse Event Reporting System (VAERS) National reporting system
Vaccine Adverse Event Reporting System (VAERS) • Detects • new or rare events • increases in rates of known side effects • patient risk factors • Additional studies required to confirm VAERS signals • Not all reports of adverse events are causally related to vaccine
AdverseEventClassification • Vaccine-induced: Due to the intrinsic characteristic of the vaccine preparation and the individual response of the vaccinee. These events would not have occurred without vaccination (e.g., vaccine-associated paralytic poliomyelitis after oral polio vaccine). • Vaccine-potentiated: The event would have occurred anyway, but was precipitated by the vaccination (e.g., first febrile seizure in a predisposed child). • Programmatic error: Due to technical errors in vaccine storage, preparation, handling, or administration. • Coincidental: The reported event was not caused by vaccination but happened by chance occurrence or due to underlying illness.
Vaccine-associatedparalyticpolio (VAPP): overallincidence of oncecase of VAPP: per 2.4 milliondoses of OPV Rotavirusvaccine/ increased risk of intussusception: no evidencefor a causallink (coins.) MMR-V: additional 4.3 febrileseizuresper 10.000 MMR-V dosescomparedto MMR and V administeredseparately MCV4/ Guillain-BarreSyndrome: no evidencefor a causal link (coincidental) Hep B V/ Guillain-BarreSyndrome, transversemyelitis: no evidencefor a causal link MMR/ autism, inflammatoryboweldiseases: no evidencefor a causal link (coinc.) Thimerosal (mercurycontainingpreservative)-containingvaccines/ autism, inflammatory boweldiseases, ADHD : no evidencefor a causal link (coincidental) Vaccines/ ITP: vaccinepotentiated