Download
1 / 1
10 likes | 113 Views
Effective Use: A Metric for Assessing the Potential Impact of HWTS Interventions Daniele Lantagne, PhD, PE and Thomas Clasen, JD, PhD London School of Hygiene and Tropical Medicine, London, UK. Department of Infectious and Tropical Diseases Disease Control and Vector Biology Unit.

E N D
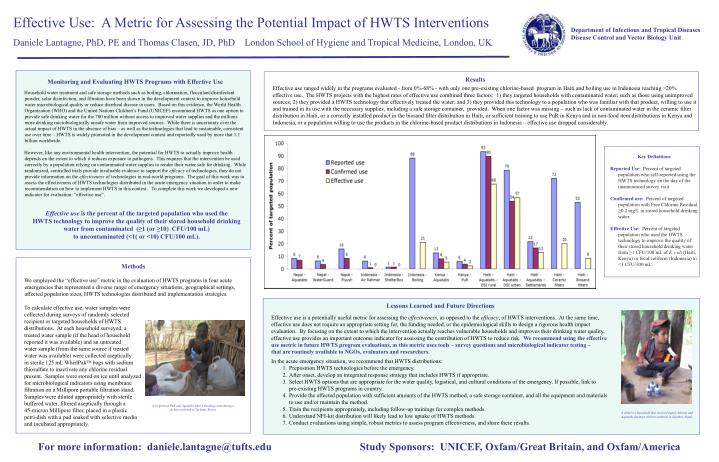
Effective Use: A Metric for Assessing the Potential Impact of HWTS Interventions Daniele Lantagne, PhD, PE and Thomas Clasen, JD, PhD London School of Hygiene and Tropical Medicine, London, UK • Department of Infectious and Tropical Diseases • Disease Control and Vector Biology Unit • Household water treatment and safe storage methods such as boiling, chlorination, flocculant/disinfectant powder, solar disinfection, and filtration have been shown in the development context to improve household water microbiological quality or reduce diarrheal disease in users. Based on this evidence, the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) recommend HWTS as one option to provide safe drinking water for the 780 million without access to improved water supplies and the millions more drinking microbiologically unsafe water from improved sources. While there is uncertainty over the actual impact of HWTS in the absence of bias – as well as the technologies that lead to sustainable, consistent use over time – HWTS is widely promoted in the development context and reportedly used by more that 1.1 billion worldwide. • However, like any environmental health intervention, the potential for HWTS to actually improve health depends on the extent to which it reduces exposure to pathogens. This requires that the intervention be used correctly by a population relying on contaminated water supplies to render their water safe for drinking. While randomized, controlled trials provide invaluable evidence to support the efficacy of technologies, they do not provide information on the effectiveness of technologies in real-world programs. The goal of this work was to assess the effectiveness of HWTS technologies distributed in the acute emergency situation in order to make recommendation on how to implement HWTS in this context. To complete this work we developed a new indicator for evaluation: “effective use”. • Effective use is the percent of the targeted population who used the • HWTS technology to improve the quality of their stored household drinking water from contaminated (≥1 (or ≥10) CFU/100 mL) • to uncontaminated (<1( or <10) CFU/100 mL). Effective use ranged widely in the programs evaluated - from 0%-68% - with only one pre-existing chlorine-based program in Haiti and boiling use in Indonesia reaching >20% effective use. The HWTS projects with the highest rates of effective use combined three factors: 1) they targeted households with contaminated water, such as those using unimproved sources; 2) they provided a HWTS technology that effectively treated the water; and 3) they provided this technology to a population who was familiar with that product, willing to use it and trained in its use with the necessary supplies, including a safe storage container, provided. When one factor was missing – such as lack of contaminated water in the ceramic filter distribution in Haiti, or a correctly installed product in the biosand filter distribution in Haiti,orsufficient training to use PuR in Kenya and in non-food item distributions in Kenya and Indonesia, or a population willing to use the products in the chlorine-based product distributions in Indonesia – effective use dropped considerably. Results Monitoring and Evaluating HWTS Programs with Effective Use • Key Definitions • Reported Use: Percent of targeted population who self-reported using the HWTS technology on the day of the unannounced survey visit. • Confirmed use: Percent of targeted population with Free Chlorine Residual ≥0.2 mg/L in stored household drinking water. • Effective Use: Percent of targeted population who used the HWTS technology to improve the quality of their stored household drinking water from ≥1 CFU/100 mL of E. coli (Haiti, Kenya) or fecal coliform (Indonesia) to <1 CFU/100 mL. We employed the “effective use” metric in the evaluation of HWTS programs in four acute emergencies that represented a diverse range of emergency situations, geographical settings, affected population sizes, HWTS technologies distributed and implementation strategies. To calculate effective use, water samples were collected during surveys of randomly selected recipient or targeted households of HWTS distributions. At each household surveyed, a treated water sample (if the head of household reported it was available) and an untreated water sample (from the same source if treated water was available) were collected aseptically in sterile 125 mL WhirlPak bags with sodium thiosulfate to inactivate any chlorine residual present. Samples were stored on ice until analyzed for microbiological indicators using membrane filtration on a Millipore portable filtration stand. Samples were diluted appropriately with sterile buffered water, filtered aseptically through a 45-micron Millipore filter, placed in a plastic petri-dish with a pad soaked with selective media and incubated appropriately. Methods • Effective use is a potentially useful metric for assessing the effectiveness, as opposed to the efficacy, of HWTS interventions. At the same time, • effective use does not require an appropriate setting for, the funding needed, or the epidemiological skills to design a rigorous health impact • evaluation. By focusing on the extent to which the intervention actually reaches vulnerable households and improves their drinking water quality, • effective use provides an important outcome indicator for assessing the contribution of HWTS to reduce risk. We recommend using the effective • use metric in future HWTS program evaluations, as this metric uses tools – survey questions and microbiological indicator testing – • that are routinely available to NGOs, evaluators and researchers. • In the acute emergency situation, we recommend that HWTS distributions: • Preposition HWTS technologies before the emergency. • After onset, develop an integrated response strategy that includes HWTS if appropriate. • Select HWTS options that are appropriate for the water quality, logistical, and cultural conditions of the emergency. If possible, link to pre-existing HWTS programs in country. • Provide the affected population with sufficient amounts of the HWTS method, a safe storage container, and all the equipment and materials to use and/or maintain the method. • Train the recipients appropriately, including follow-up trainings for complex methods. • Understand NFI-kit distribution will likely lead to low uptake of HWTS methods. • Conduct evaluations using simple, robust metrics to assess program effectiveness, and share these results. Lessons Learned and Future Directions A recipient of PuR and Aquatabs after a flooding event during a cholera outbreak in Turkana, Kenya. A child in a household that received liquid chlorine and Aquatabs during a cholera outbreak in Jajarkot, Nepal. For more information: daniele.lantagne@tufts.edu Study Sponsors: UNICEF, Oxfam/Great Britain, and Oxfam/America