Download
1 / 13
270 likes | 1.75k Views
A-SCAN INSTRUMENT. INTRODUCTION. Ultrasound is a high frequency sound that you cannot hear, but it can be emitted and detected by special machines.

E N D
INTRODUCTION Ultrasound is a high frequency sound that you cannot hear, but it can be emitted and detected by special machines. Ultrasound travels freely through fluid and soft tissues. However, ultrasound is reflected back (it bounces back as 'echoes') when it hits a more solid (dense) surface. For example, the ultrasound will travel freely though blood in a heart chamber. But, when it hits a solid valve, a lot of the ultrasound echoes back. Another example is that when ultrasound travels though bile in a gallbladder it will echo back strongly if it hits a solid gallstone.So, as ultrasound 'hits' different structures in the body of different density, it sends back echoes of varying strength.
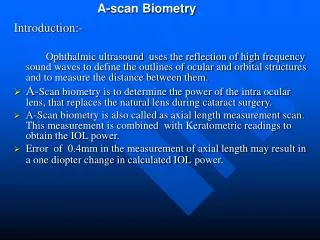
A-SCAN INSTRUMENT A-Scan ultrasound biometry, commonly referred to as an scan, is routine type of diagnostic test used in ophthalmology. This equipment provides data on the length of the eye, which is a major determinant in common sight disorders. The most common use is to determine eye length for calculation of intraocular lens power. Briefly, the total refractive power of the emetropic eye is approximately 60. Of this power, the cornea provides roughly 40 diopters, and the crystalline lens 20 diopters. When a cataract is removed, the lens is replaced by an artificial lens implant.
A-SCAN INSTRUMENT By measuring both the length of the eye and the power of the cornea (keratometry), a simple formula can be used to calculate the best fit of intraocular lens. There are several different forumlas that can be used depending on the actual characteristics of the eye. The other major use of the A-Scan is to determine the size and ultrasound characteristics of masses in the eye, in order to determine the type of mass. Instruments used in this type of test require direct contact with the cornea, however a non-contact instrument has been reported. Disposable covers, which come in actual contact with the eye, have also been evaluated.
Reflectivity The A-scan probe projects a thin sound beam that travels through liquid or tissue. When the sound beam encounters the interface of a substance that is dissimilar from the substance it is traveling through, part of the sound beam energy is reflected, and part of the sound energy projects through the new substance. The more dissimilar the substances are, the stronger the reflection, or echo, is.
Reflectivity When the A-scan beam is projected into the phakic (natural lens) eye it travels through the aqueous humor and encounters a dissimilar substance in the anterior lens surface. Energy is reflected back to the transducer in the probe tip. The instrument displays the intensity of the reflection as a spike above the baseline (which represents distance) on a graph. Strong reflections also occur as the sound beam encounters the posterior lens surface and the retina. Spikes representing these reflections appear at their corresponding positions along the baseline. The first spike represents the probe tip as it comes into contact with the cornea.
Corneal compression Since ultrasound does not travel through air, the A-scan probe must come into contact with the cornea, either directly or through a liquid. If a corneal-contact method is used, there is a danger of the probe putting too much pressure on the cornea, causing the cornea to compress, which results in an artificial shortening of the axial eye length. This is a significant potential error source. A .4mm compression error can result in a 1 diopter error in the calculated IOL power.
Evaluating the scan: Is the measurement accurate? Special care must be taken when performing pseudophakic scans because of the presence of reverberation echoes. Your instrument may mistake one of these echoes for the retina echo and produce an inaccurate axial length. The figure to the right depicts anterior (A) and posterior (B) lens echoes from an IOL and two reverberation spikes (C, and D).
** Some instruments use measuring "gates" that measure the first spike to reach a threshold height within a specified distance along a baseline. Make sure a reverberation spike does not appear within the retina gate. In the figure to the right a reverb spike is within the retina gate at point A. The gate would need to be moved or resized to avoid this spike. Otherwise the instrument will read the spike at point A as being the retina spike.
** Some instruments use "lights" that attach to spikes that reach a threshold height, no matter where they occur on the baseline. In the aphakic mode there may only be two lights; one for the cornea, and one for the retina. Make sure the retina light attaches to the retina spike and not a reverb spike. In the figure to the right the retina light has attached to a reverb spike (A). You will need to manually move it to the retina spike (B). It is sometimes easier to identify reverberation spikes if the gain is turned down. The manual to your instrument will tell you how to adjust gates or move lights, if necessary.
** Sometimes cataract surgery results in a post-operative refractive "surprise". Perhaps we were aiming for plano and the eye ended up with a -3.00 D refractive error. In these cases we would like to pinpoint the cause of the error. We will want to confirm that the axial length was correctly measured.
** It is always a good idea to have K readings and A-scan measurements on both eyes before cataract surgery is performed. Since both eyes have similar measurements in most people, this provides a double-check of the measurement. If the fellow eye has an IOL inserted by another doctor, you may not have access to the IOL specifications and/or the measurement information.
** It is sometimes necessary to replace an IOL that was inserted many months or years ago. Even if you have IOL specifications and measurement information from the previous surgery, it is nice to have the confirmation of a current measurement. It is necessary to have a new measurement if a scleral buckling procedure, which lengthens the eye, has been done since the IOL was inserted.