Download
1 / 10
100 likes | 308 Views
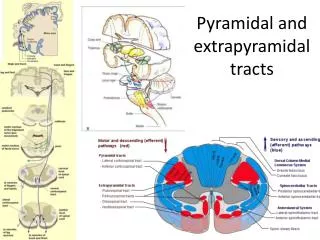
Motor tracts Chris Lancaster and Joshua Bower Questions: c.j.lancater@warwick.ac.uk J.Bower@warwick.ac.uk. Motor tracts . Lateral corticospinal tract Ventral corticospinal tract Rubrospinal tract Vestibulospinal tract Reticulospinal tracts.

E N D
Motor tracts Chris Lancaster and Joshua Bower Questions: c.j.lancater@warwick.ac.uk J.Bower@warwick.ac.uk
Motor tracts Lateral corticospinal tract Ventral corticospinal tract Rubrospinal tract Vestibulospinal tract Reticulospinal tracts
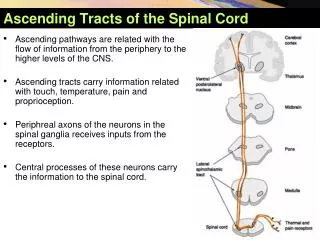
What do the Reticulospinal tracts affect? - Either inhibits or excites lower motor neurons - Modulate muscle activity/tone – especially in antigravity muscles - Modulate sympathetic activity - Control emotional movement of muscles of facial expression Patients can smile even if they have bilateral corticobulbar lesions to CN VII
corticospinal, rubrospinal, vestibulospinal, reticulospinal What do the Rubrospinal and Vestibulospinal tracts influence? Rubrospinal tract- flexor tone Vestibulospinal tracts- extensor muscle tone What are reticulospinal nuclei and tracts involved in (2 marks)? What are the two main nuclei? Locomotion and posture- involved in extensor reflex Pedunculopontine nucleus = main locomotion centre Communicates with pontine and medullary nuclei
Describe the cranial nerve motor supply from the cortex • Bilateralsupply from cortex • Innervation comes from corticobulbar/corticonuclear neurons • Main UMN innervation is contralateral • So cortex damage results in weakness but not total paralysis. • Can then recover as ipsilateral UMNs compensate. • Decussation occurs at synapse on to CN LMN in the brain stem • MAIN EXCEPTION = Unilateral supply to CN VII to the lower face
What are the signs of Lower motor neuron lesions? • Muscle wasting • Fasciculation's • Hyporeflexia • Flaccid paralysis
What are the signs of upper motor neuron lesion • Spastic paralysis • Hyperreflexia • No muscle wasting • Extensor plantar response