Download
1 / 63
760 likes | 1.94k Views
DIAPHRAGM AND HIATUS HERNIA. Anatomy of diaphragm. Diaphragm Diaphragmatic communications. Physiology. Normal anatomy of LES. Normal anatomy of LES. Normal anatomy of LES. Hernia-peritoneum diverticulum. Clasification. Congenital Accuired. Congenital hernia.

E N D
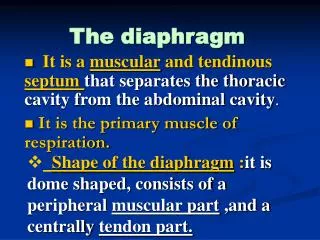
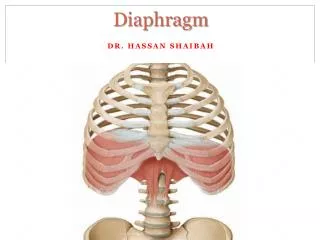
Anatomy of diaphragm • Diaphragm • Diaphragmatic communications
Clasification • Congenital • Accuired
Incidence • 1 : 2000-5000 live birth • 8 % of all major congenital anomalies • mortality rate nearing 70 percent • CDH accounts > 1% of total infant mortality in USA • Cost per new case CDH = 250 000 $
Causes • The cause of CDH is largely unknown • CDH can occur as part of a multiple malformation syndrome • Karyotype abnormalities have been reported in 4% of infants with CDH
Congenital Diaphragmatic Hernias (CDH) • Types of Congenital Diaphragmatic Hernias (CDH) • Bochdalek • Morgagni • Diaphragmatic eventration • Central tendon defects
Bochdalek Hernia • Postero-lateral diaphragmatic hernia • Most common manifestation of CDH, accounting for more than 95% of cases • Majority of Bochdalek hernias (80-85%) occur on the left side of the diaphragm • A failure of the diaphragm to completely close during development. • Herniation of the abdominal contents into the chest • Pulmonary hypoplasia
Morgagni Hernia • anterior defect of the diaphragm • referred to as Morgagni’s, retrosternal, or parasternal hernia • accounts for approximately 2% of all CDH cases • characterized by herniation through the foramina of Morgagni which are located immediately adjacent to the xyphoid process of the sternum • majority occur on the right side of the body and are generally asymptomatic
Diaphragmatic eventration • abnormal displacement (i.e. elevation) of part or all of an otherwise intact diaphragm into the chest cavity • diaphragm is thinner in the region of eventration, allowing the abdominal viscera to protrude upwards • thinning is thought to occur because of incomplete muscularisation of the diaphragm • Minor forms of diaphragm eventration are asymptomatic
Congenital Diaphragmatic Hernias (CDH) • Left sided CDH is a 2 - 4 cm postero-lateral defect • Right lobe of liver can occupy most of hemithorax in rt side defect • Hepatic veins may drain ectopically into right atrium • Lung and liver may be fused
Prenatal Diagnosis • ultrasonography diagnosis(as early as the second trimester) * bad prognosis
Prenatal MR Imaging - single-shot turbo spin-echo (HASTE)- of congenital diaphragmatic hernia
Prenatal Counselingmultidisciplinary team • patient's obstetrician • perinatologist • geneticist • surgeon • social worker
Prenatal management • Glucocorticoids • Thyrotropin-releasing hormone • Fetal surgical therapy (Antenatal surgical intervention, In utero tracheal occlusion)
Delivery Room Management • affected infants should be delivered in a specialized center • require positive pressure ventilation in the delivery room. • to prevent distension of the gastrointestinal tract and further compression of the pulmonary parenchyma, a double-lumen nasogastric or orogastric tube of large caliber is placed to act as a vent. • early intubation
Postnanal Diagnosis • Respiratory distress • Scaphoid abdomen • Auscultation of the lungs reveals poor air entry • Shift of the heart to the side opposite
Postnanal Diagnosis left-sided CDH • Radiograph in a male neonate shows the tip (large arrow) of the nasogastric tube positioned in the left hemithorax. Note the marked apex leftward angulation of the umbilical venous catheter (small arrow).
Right congenital diaphragmatic hernia • Radiograph in a male neonate shows that the nasogastric tube (arrow) deviates to the left of the thoracic vertebral bodies as it passes through the inferior portion of the thorax
Postnatal management • Mechanical ventilation • Nitric Oxide • Surfactant • Surgery
Evolving Therapies • In utero repair • Liquid ventilation • Pulmonary transplantation • Pharmacology • Prostacyclin derivatives • Calcium channel blockers • Phosphodiesterase inhibitors
Prognosis • Pulmonary recovery: When all resources, are provided, survival rates range from 40-69%. • Long-term morbidity: Significant long-term morbidity, including chronic lung disease, growth failure, gastroesophageal reflux, and neurodevelopmental delay, may occur in survivors.
Classification • ?Asymptomatic congenital diaphragmatic hernia • Posttraumatic or postoperative • Hiatus hernia
Symptoms • Uncomplicated: • Similar woth GERD • Respiratory symptoms • Cardiac arrhythmia, ischemic heart disease\ • Complications: • Strangulation: acute respiratory and digestive symptoms, very difficult to assess on clinical examination
Diagnostic • Plain thoracic X-Ray • Nasogastric tube + X-ray • Barium or Gastrographin studies if non-emergency • CT-scan
Treatment • Approach: • Laparotomy vs laparoscopy • Thoracotomy vs thoracoscopy • Urgent vs chronic disease • Reintegration of viscus • Resection of peritoneal sac • Close the defect in diaphragm • Suturing • Mesh
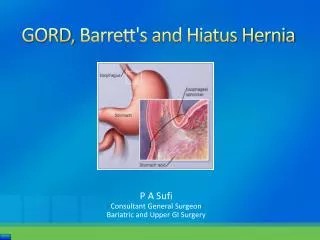
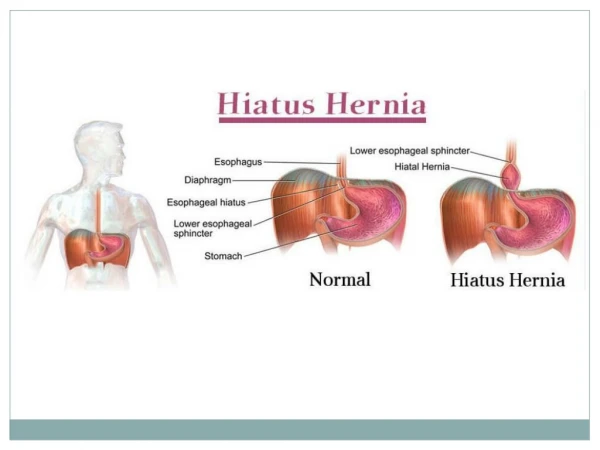
Hiatal Hernia Defined (Also called Diaphragmatic Hernias) Protrusion of the stomach upward into the mediastinal cavity through the esophageal hiatus of the diaphragm Sliding 90% of cases Rolling (paraesophageal)
Sliding Hiatal Hernia The esophagus passes through the diaphragm and connects to the stomach. When a sliding hiatal hernia is present, part of the stomach moves up through an opening (hiatus) in the diaphragm. The presence of a hiatal hernia increases the risk for gastroesophageal reflux
Paraesophageal Hiatal Hernia The fundus and possibly portions of the stomach’s greater curvature, rolls through the esophageal hiatus and into the thorax beside the esophagus
A Comparison of the normal stomach, sliding hiatal hernia and rolling hiatal hernia
Diagnostic Tools Barium Swallow CXR Endoscopy with biopsy Stool for quiac Esophageal manometry