Download
1 / 8
80 likes | 371 Views
Acute sore throat. What else might it be? Prodigy. Infectious mononucleosis (glandular fever) Epiglottitis (requires urgent admission) Thyroiditis Gonococcal pharyngitis (rare) Diphtheria (very rare in the UK)

E N D
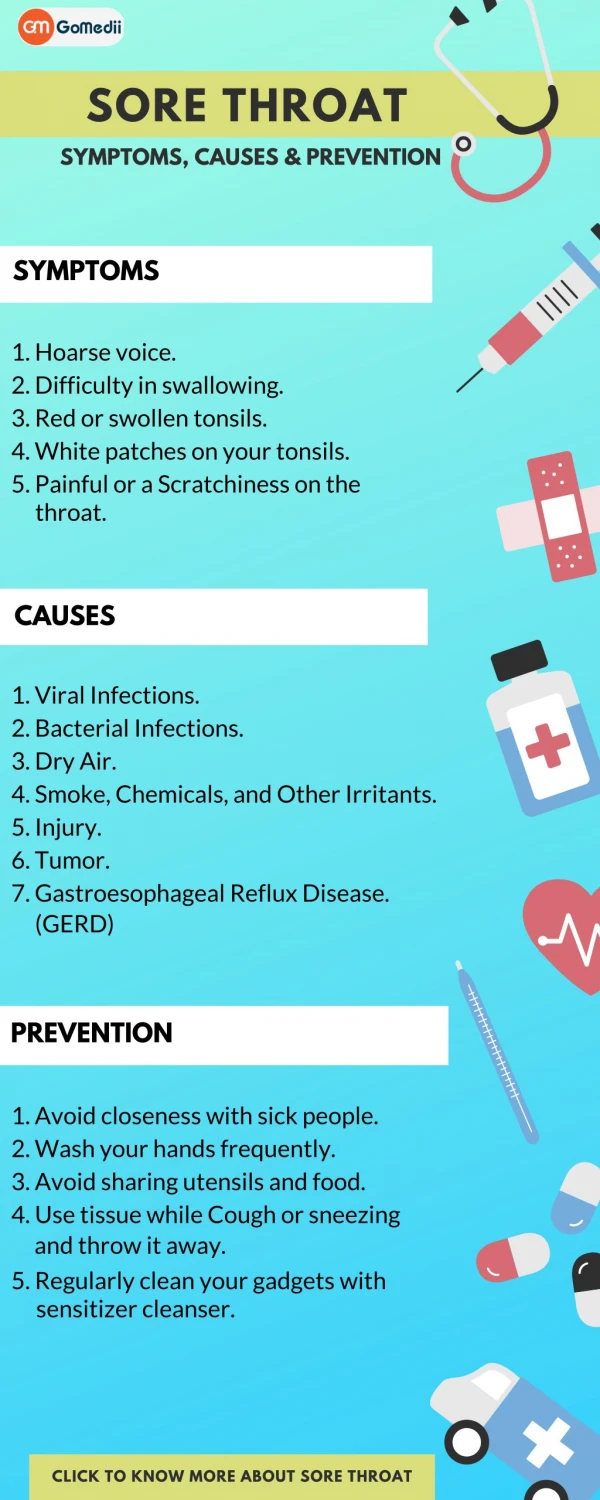
What else might it be?Prodigy • Infectious mononucleosis (glandular fever) • Epiglottitis (requires urgent admission) • Thyroiditis • Gonococcal pharyngitis (rare) • Diphtheria (very rare in the UK) • Neutropenia (ensure the person is not on medication known to cause immunosuppression)
Temp > 38c 1 Absence of cough 1 Swollen, tender anterior cervical nodes 1 Tonsillar swelling or exudate 1 Score : If 0 then <1% chance of Strep (Group A Beta Haemolytic Streptococcus) If 3 of 4 approx 40% chance of Strep (Group A Beta Haemolytic Streptococcus ) Sore throat Clinical Prediction Rule 1Centor RM, et al. Med Decision Making 1981; 1: 239–46
Clinical Prediction Rule 2McGinn TG, et al. Mayo Clin Proc 2003; 78: 289–93 Score Per cent with GABHS (95% CI) -1 5% (0–12) 0 16% (7–30) 1 44% (28–62) 2 57% (29–82) 3 83% (36–100) • Validated in a cohort of 171 consecutive walk in patients. Overall prevalence of GABHS was 24% • Temp > 38.3C = 1 point; Cough = -1 point; presence of pharyngeal or tonsillar exudates = 1 point; enlarged or tender anterior cervical lymph nodes = 1 point; close contact with someone believed to have strep infection = 1 point.
Treatment options for sore throat?. Antibiotics Cochrane review. Del Mar CB, et al. Issue 3. 2004 (26 RCTs; 11,452 cases) Symptoms(headache, soreness and fever): reduced to half at day 3 Non-suppurative complications: trend to less glomerulonephritis (insufficient cases) and reduced rheumatic fever to one third (from older trials) Suppurative complications: reduced complications of otitis media (NNT = 87), acute sinusitis (NNT = 175) and quinsy (NNT = 46) Analgesia Clinical Evidence. Del Mar C and Glazsiou P. Search date 2004 Ibuprofen reduced throat pain at < 24hrs and 2–5 days In two RCTs, a single dose of paracetamol reduced sore throat pain at 2–3 hours compared with placebo, and in another paracetamol three times daily reduced pain at 2 days
Antibiotics of limited value in sore throat? Little P. BMJ 1997;314:722–6 716 patients. Compared 10 day antibiotic prescription, no prescription and delayed prescription (3 days) Antibiotic associated with slightly reduced fever but no difference in number of days of illness, days off work or patients better at day 3. Zwart S, et al. BMJ 2003:327:1324–7 308 children. Compared 4 day and 7 day Pen V with placebo. (severely ill excluded) No significant difference in duration of sore throat. Of 96 with positive GABHS throat swab, Pen V for 7 days also made no significant difference Concludes: no rationale exists for treatment with antibiotics in most children with sore throat Rare complicationse.g. rheumatic fever, peritonsillar abscess, mastoiditis. Very rare reports and overall rates remain steady despite reduced antibiotic prescribing (mastoiditis - increased hospital admissions and corresponding reduced GP episodes) Sharland M, et al. BMJ 2005; 331: 328–29
Delayed prescription? Maybe a useful management strategy. Little P. BMJ 1997;314:722–6 69% given delayed prescription did not receive antibiotics More patients given antibiotics returned with subsequent sore throat (NNT = 9) “To avoid medicalising a self-limiting illness doctors should avoid antibiotics or offer a delayed prescription for most patients with sore throat”
Sore throatSummary • Identify any differential diagnosis • Undertake risk assessment for GABHS • Antibiotics may make no difference to those not severely ill, even if they have GABHS (Zwart S, 2003) • Analgesia may help with sore throat pain • Weigh up benefits versus risks of any antibiotic treatment • If clinician concern (e.g. assessed high risk of severely ill), or patient / parental pressure to prescribe, consider a delayed prescription (Little P, 1997)