Download
1 / 45
510 likes | 654 Views
Learn about the clinical indications, monitoring, and pharmacokinetics of teicoplanin and vancomycin, with a focus on mechanisms of action and resistance. Discover appropriate and inappropriate uses, along with the importance of pharmacokinetics/pharmacodynamics for optimizing treatment.

E N D
Teicoplanin and vancomycin:clinical indications and usefullness of drug monitoring Profs B. Vandercam, P. Wallemacq & P.M. Tulkens Cliniques universitaires Saint-Luc & Université catholique de Louvain,Brussels, Belgium http://www.md.ucl.ac.be/seminfect Séminaire de Pathologie Infectieuse - 26 octobre 2000
Teicoplanine et vancomycin…what are we going to tell you ? • Mode of action and mechanisms of resistance • Acceptable clinical indications • Monitoring: what to do and why ? • Pharmacodynamics / Pharmacokinetics • And then what to do ... UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
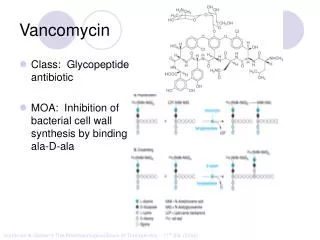
N-acetylglucosamine N-acetylmuramic acid Undecaprenyl lipid carrier Mode of action : inhibition of bacterial cell wall synthesis upstream to lactams CELL WALL -L-Ala-D-Glu-L-Lys-D-Ala-D-Ala -L-Ala-D-Glu-L-Lys-D-Ala NH -L-Ala-D-Glu-L-Lys-D-Ala-D-Ala -L-Ala-D-Glu-L-Lys-D-Ala-D-Ala transpeptidase NH2 -L-Ala-D-Glu-L-Lys-D-Ala-D-Ala transglycosylase NH2 - L-Ala-D-Glu-L-Lys-D-Ala-D-Ala CYTOPLASM L-Ala D-Ala D-Ala:D-Ala ligase D-Ala-D-Ala NH2 L-Lys-D-Glu-L-Ala- -UDP NH2 D-Ala-D-Ala-L-Lys-D-Glu-L-Ala- -UDP NH2 D-Ala-D-Ala-L-Lys-D-Glu-L-Ala- lactams UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Binding of vancomycin to D-Ala-D-Ala UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Vancomycin used resistance Relationship between the use of vancomycin and the development of resistance in enteroccci in U.S.A. 14 45 40 12 35 10 30 8 25 Vancomycin used (kg) % resistance 20 6 15 4 10 2 5 0 0 1987 1988 1989 1990 1991 1992 1993 1994 UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
1.3% 1.4% 2% 0.6% 4.2% 3.1% 0.9% 3.5% 3.9% Brown and Courvalin, ICAAC, 1996 Resistance to glycopeptides in Europe ... UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
North America no use of avoparcin in animals low animal reservoir large use in clinics selection in patients curb/restrict usage but isn’t too late ?? Europe large use of avoparcin in animals large animal reservoir low use in clinics no selection in patients maintain low usage it IS still time …. Why different levels in North America and Europe ? UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Resistance to vancomycin in enterococci (VRE) and staphylocci (GISA): the real issues... • microorganisms with high-level resistance to penicillin and aminoglycosides and dubious sensitivity to most “classical” antimicrobials • treatment options • combinations of antimicrobials • experimental compounds with unproven efficacy • new compounds (synercid, linezolid, …) which we may loose quickly... UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Glycopeptides appropriate uses • serious infections due to beta-lactam- resistant gram-positive microorganisms • infections due to gram-positive microorganisms in patients with serious allergy to beta-lactam antimicrobials • antibiotic-associated colitis (AAC) non- responding to metronidazole or potentially life-threatening • prophylaxis for endocarditis in patients at high risk • prophylaxis for major surgical procedures see meta-analysis…. UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Vancomycin in S. Aureus endocarditis(Levine, Ann Intern Med 1991) • Bacteremia > 9 days • Bacteriostatic / slow Use glycopeptides only if • resistance • toxicity
Comparative efficacy and safety of teicoplanin and vancomycin Wood, JAC 1996) Meta-analysis of 11 clinical trials (1276 pts) Direct comparisons difficult Teicoplanin as effective as vancomycin Teicoplanin superior tolerability (?) Teicoplanin advantages : - once daily, bolus - intramuscular - cost monitoring (cost more but do less !!!) UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Glycopeptides inappropriate uses (1/2) Treatments • empiric in febrile neutropenia (except high suspicion of MRSA) • single blood culture positive for coagulase-negative staphylococcus • cultures negative for beta-lactam- resistant Gram(+) organisms • primary treatment of antibiotic associated colitis (AAC) • topical application or irrigation UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Glycopeptides inappropriate uses (2/2) Prophylaxis • routine prophylaxis in • surgery (except in beta-lactam allergy) • very low-birth-weight infants • peritoneal dialysis or hemodialysis • infection or colonization of indwelling central or peripheral intravascular catheters • eradication of MRSA colonization • selective decontamination of the digestive tract UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Can pharmacokinetics/pharmacodynamics help in optimizing glycopeptide treatments ? • efficacy (primary end-point) • prevention of emergence of resistance(secondary but crucial endpoint) UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
AUC / MIC ratio But, what is this ? Glycopeptides PK/PD: which is the important parameter ? • slowly cidal • time-dependent killing • long half-life UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Area under the curve (AUC) dependent on the total dose and half-life UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
AUC / MIC ratio dependent on the total dose, half-life and MIC UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
AUC vs peak and trough In a given schedule, • peak and trough levels, and • AUC are directly correlated • to one another • to the dose • to the inverse of the clearance UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
30 1g 15 0.5g AUC= 200 8 7.5 AUC= 100 4 0.25 g AUC= 50 2 Peak, trough, and AUC are interelated... An example with vancomycin... 30 10 Vancomycin serum concentration 3 1 0 12 Time (hours) UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Glycopeptides monitoring : practical aspects for the clinician • blood drawing on dry tubes or on EDTA • before infusion (trough level) • 2h after the end of the infusion ( “peak” level) Take care to: • avoid contamination from the infusion line • note the drawing time, start/end of infusion, ... • indicate the dose and the dose interval • communicate the patient’s specifics (age, height, weight, creatinine, underlying pathologies, etc…)... UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Glycopeptides monitoring : how do we do it for you ? • immuno-assays (Abbott TDM, Dade-Behring, BMD…) • duration of the assay: 15 min • interpretation using TDM-PK software (one-compartment or more sophisticated programs…) • duration of the PK protocol: 5-10 min/patient • direct costs: 100 (vanco) - 300 (teico) BEF/test • INAMI / RIZIV refunding: 300,- BEF / isolated test or 900.- BEF/ full PK analysis UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Vancomycinstart with 1 g / 12 h and then: peak (t0)25-35 mg/L trough 5-10 mg/L AUC 200 mg/L x h-1 AUC24h400 mg/L x h-1 Glycopeptides dosingrecommendations at the Cliniques Saint-Luc Teicoplanin start with 12 mg / kg x d-1 and then : peak(t0)40-50 mg/L trough 15-20 mg/L AUC24h 560 mg/L x h-1 UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Cost-effectiveness of antibiotic full PK monitoring: two examples with aminoglycosides (1 of 3) 1. US studies (Crist et al 1987; Destache et al 1990) • Two prospective, randomized studies with • 75/118 adult patients with monitoring and full PK analysis ( = TDM/PK), vs • 70/103 patients with isolated blood level determinations (no PK analysis; = control) • homogenous groups in age, sex, size, pathogens, infected sites, Apache II score... UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Cost-effectiveness of antibiotic full PK monitoring: two examples with aminoglycosides (2 of 3) US studies UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Cost-effectiveness of antibiotic full PK monitoring: two examples with aminoglycosides (3 of 3) 2. European study(Vincks et al. 1999) • 105 patients followed by active PK-guided monitoring (ATDM), vs • 127 followed by non PK-guided monitoring (TDM) • statistical improvements by ATDM vs TDM (p<0.01): • higher peaks (10.6 vs 7.6 mg/L) • lower trough (0.7 vs 1.4 mg/L) • shorter hospital stay (12.6 vs 18 days) • lower incidence of nephrotoxicity (2.9 vs 13.4 %) • lower total costs (NGL 8,883 vs 11,743) UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Total cumulative doses of vancomycin based either on the initial dose regimen extrapolated to the duration of treatment (median 21d) or on the dose adjusted by TDM-PK (Clin. Univ. St Luc) You do reduce theoverall usage ... UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Monitoring and prevention of toxicity:effect of age on vancomycin nephrotoxicity risk (1/2) • Data base of 11471 vancomycin files (St Luc) • Exclusion criteria: • error or suspicion in the blood drawing • renal insuf (ser creat. >2.5 mg/dL) • child < 6 yr, and adults between 40 et 65 yr • Selection criteria (n = 111): • complete files: peak conc., trough levels, creatinine, body weight… • trough > 10 µg/mL min. 4 days UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Monitoring and prevention of toxicity:effect of age on vancomycin nephrotoxicity risk (2/2) 72 reduct. Clcr 27% 73 yr 16.6µg/ml 111 patients with trough >10 µg/ml (min.4 days) p = 0.05 39 reduct. Clcr 11% 15.8µg/mL 20 yr UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Peak/MIC= 3.75 24h-AUC/MIC = 50 MIC = 8 Peak/MIC= 15 24h-AUC/MIC = 200 MIC = 2 Peak/MIC= 60 24h-AUC/MIC = 800 MIC = 0.5 Peak, trough and 24h-AUC must be examined in relation to the MIC... Vancomycin 1 g every 12h : 2 pks of 30 µg/ml in 24 h 24h-AUC= 400 30 8 Vancomycin serum concentration 2 0.5 0 12 Time (hours) UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Vancomycin Outcomes vsMIC and AUC/MICs Outcome Satisfactory Unsatisfactory Indeterminate MIC >1.0 µg/ml 1 4a 0 MIC <1.0 µg/ml 74 2 3 AUC / MIC <125 4 4b 0 AUC / MIC >125 71 2 3 Total Patients (84) 75 6 3 ap < 0.001 bp < 0.005 Hyatt, et al. Clin Pharmacokinet. 1995;28:143-160. UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Vancomycin 1g every 12h (normal adult)PK/PD parameters for 1g every 12h MIC Peak/MIC 24h-AUC/MIC 1 30 400 2 15 200 4 7.5 100 8 3.75 50 UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
24h-AUC / MIC > 101 24h AUC / MIC < 100 24h-AUC/MIC and Resistance 100 75 50 Probability of remaining susceptible 25 0 0 5 10 15 20 Days from initiation of therapy Thomas JK. Antimicrobial Agents Chemother 1998;42:521–527. UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
24h-AUC/MIC <400 (n=16) P=0.0402 24h-AUC/MIC >400 (n=18) Vancomycin “time to eradication” in MRSA Infections 100 80 60 Percent Culture Positive 40 20 0 0 10 20 30 Day of Eradication Moise, Forrest & Schentag. Submitted, 2000. UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Why is vancomycin so weak vs MRSA? • Slowly or poorly cidal, hetero-resistance? • MIC test is incorrect • PK/PD “golden target” of a 24h-AUC / MIC of 125 (viz. the fluoroquinolones) is too low… should be 400 or even more ??? • Protein Binding of vancomycin, lowering effective AUC ? • MBC >> MIC for these vancomycin exposed organisms? UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
with 50 % protein binding... total 24h-AUC= 400 Can get an MIC of > 2, can’t you ? free “useful” 24h-AUC= 200 MIC may perhapsnot exceed 1 ... Vancomycin 1 g every 12h 30 10 Vancomycin serum concentration 1.0 0 12 Time (hours) UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Vancomycin /Teicoplanin PK/PD parameters taking into account protein binding protein half 24h-AUC * MIC binding life total “free” ** max * (%) (h) mg/L xh-1 mg/L vancomycin 10- 50 % 6 400 200 1- 2(1g / 12h) teicoplanin 90 > 40 560 56 0.5 (6 mg/kg in 24h) *values directly proportional to the dose **in vitro and animal PK/PD studies of most antibiotics show that only free drug is active UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Clinical outcome / teicoplanin predose concentration Mc Gouwan, J Inf Chemother 1996-1998Harding, JAC 2000 Wilson , IJAA 1994) S. aureus septicemia (n = 80) Success rate : 20 % if Cmax < 5 mg/L 90 % if Cmax > 25 mg/L S. aureus endocarditis (n = 21) Success rate : 40 % if Cmax < 20 mg/L 91 % if Cmax > 20 mg/L UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Teicoplanin recommanded levels • common indications : trough > 10 mg/l 6 mg / (kg x d) • for S. aureus septicemia, S. aureus endocarditis, osteoarthritis, … trough > 20 mg/l 12 mg / (kg x d) • if every other day 18 mg / kg every 48 h CLINICAL EXPERIENCE ... UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Conclusions (1/3) ... • Both vancomycin and teicoplanin should be used restrictively !! • If needed, both should be administered correctly • Monitoring is beneficial if associated with a full PK analysis • avoidance/correction in errors of administration • decreased incidence of side effects • increased efficacyTrue monitoring is never a single determination !! We need MIC’s... UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Conclusions (2/3) ... In the absence of etiologic diagnostic or knowledge of likely MIC: use vancomycin at full dose (1 g / 12h) and consider monitoring in • elderly • concurrent nephrotoxic drugs • prolonged course ( > 1 week) • patients necessitating high doses (high MIC, PK abnormal.) • patients with rapidly changing renal function but creatinine may do the job • but DO monitor in • patients with suspected abnormal Vd or Cl • anephric patients (hemodialysis) • ICU patients with dobutamine, dopamine, furosemide, hemofiltration, burns, IVDU UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Conclusions (3/3) ... In the absence of etiologic diagnostic or knowledge of likely MIC … teicoplanin should probably be used • at 6 mg / (kg x d) only with suspected sensitive organisms (MIC < 0.5 g/L) and non-life-threatening situations; • at 9 or even 12 mg / (kg x d) in severe cases (S. aureus sepsis, …), but lack of well-controlled clinical trials UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
Thank you ... Data for this presentation were obtained from • P. Courvalin, MD *(Institut Pasteur, Paris) • W.A. Craig, MD *(Div. Infect. Dis., Univ. of Wisconsin, Madison, WI) • J.J. Schentag, Pharm D (Pharmacokinetic Laboratory, Millard Fillmore Hosp, Buffalo, NY) • and from the authors cited in reference ---------- * previous speakers at the Séminaire de pathologie infectieuse UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000
But do not forget ... http://www.md.ucl.ac.be/seminfect and do not hesitate to ask questions…. There are no stupid questions ! UCL - Séminaire de Pathologie Infectieuse - 26 oct 2000