Download
1 / 37
370 likes | 517 Views
ASSESSING THE BREASTS. NUR211 Kathleen Hancock. Outcomes. Obtain a breast history. Perform a breast physical assessment. Document breast assessment findings . Identify pertinent breast history questions. (Continued). Outcomes.

E N D
ASSESSING THE BREASTS NUR211 Kathleen Hancock
Outcomes • Obtain a breast history. • Perform a breast physical assessment. • Document breast assessment findings. • Identify pertinent breast history questions. (Continued)
Outcomes • Identify actual/potential health problems stated as nursing diagnosis. • Differentiate between normal and abnormal findings.
Breast Composition • 3 types of tissue: • *Glandular • *Fibrous • *Adipose
Structures • Lobes and lobules • Lactiferous ducts and sinuses • Areola • Montgomery’s glands
Structures • Nipple • Cooper’s ligament • Pectoralis major and serratus anterior muscles
FunctionsWhat are the functions of… Lobes & lobules: Contain acini cells that produce milk Lactiferous ducts & sinuses: Carry and store milk Areola: Dark tissue surrounding nipple (Continued)
FunctionsWhat are the functions of… Montgomery’s glands: Sebaceous gland Nipple: Nursing and sexual stimulation Cooper’s Ligament: Ligament attached to chest wall muscles that supports breasts (Continued)
FunctionsWhat are the functions of… Pectoralis major & serratus anterior muscles: Breast overlies these muscles Lymph nodes: Drain breast, chest, and arms
Breast Health:Cancer Prevention • Self Breast Exam (SBE) • Every month • Mammogram • After age 50 every year • More frequent if personal or family history • 40-49 years every 1-2 years • Breast Exam by nurse or doctor every year
DevelopmentalVariations What developmental breast variations might be seen with: • Children • Pregnant clients • Older adults
HistoryWhat can the history tell you about the breast? • Biographical data • Current health status • Past health history • Family history • Review of systems • Psychosocial history
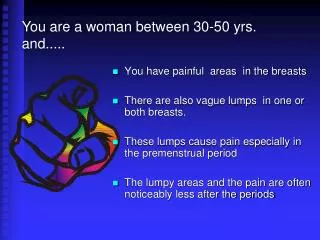
SymptomsWhat symptoms signal a problem with the breasts? • Breast lump or mass • Pain or tenderness • Nipple discharge
Physical Assessment Anatomical landmarks: quadrants of the breast, include Tail of Spence Approach: inspection, palpation (vertical, wedge, or circular) light, medium, and deep (Continued)
Physical Assessment Position: sitting, hands on hips, hands over head, leaning forward, and supine with pillow under shoulder Tools: small pillow or towel, ruler, gloves, slide, and culture slide. General survey and head-to-toe scan
Inspection Breasts: size, shape, symmetry, color, lesions, venous pattern, dimpling, or retraction Nipple and areola: nipple position and direction; discharge Axillae: color, lesions, rashes
Palpation Lymph nodes: axillary, epitrochlear, clavicular while sitting Breasts: consistency, masses, tenderness in supine position Nipple: elasticity, masses, tenderness, discharge
Supine with shoulder support –Use pads of fingers of dominant hand
Strip Method of Palpation • Cover all of breast • Use 3 middle finger pads, not tips • Use sliding motion • Overlapping dime size circles • 3 pressure levlels: light, medium, deep • Include nipple and areola
Large Breasts • Bimanual palpation to adequately examine all areas • Often have an intramammary ridge
Male Breast • Palpation • Inspection • Lymph nodes while sitting • Breast while sitting or if large while lying down
Male Breast Enlargement: • Gynecomastia
Characteristics of Masses Note: • Size Shape • Mobility Tenderness • Consistency Delimitation • Temperature Redness
Example: Pertinent Physical Findings • Right breast larger than left • No dimpling, retraction • Small, pea size (0.5cm), movable, rubbery, smooth-edged lesion in right breast at 2 o’clock in RUQ • No palpable nodes