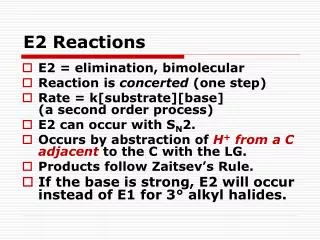
Download
1 / 30
300 likes | 534 Views
The “Emerging Paradigm” Revisited. Dov Chernichovsky, Ben Gurion University of the Negev & World Bank “Innovations in Health Financing” International Conference in Honor of Juan Luis Londono Mexico, April 20-21, 2004. Objectives of Presentation.

E N D
The “Emerging Paradigm” Revisited Dov Chernichovsky, Ben Gurion University of the Negev & World Bank “Innovations in Health Financing” International Conference in Honor of Juan Luis Londono Mexico, April 20-21, 2004
Objectives of Presentation • Articulate a political-economic framework for health system reform, based on trends over the last two decades • Use the framework to • Relate to Israeli (and Mexican) reform efforts • suggest potential future directions Chernichovsky - draft - dov@mail.bgu.ac.il
Structure of Talk • Features of the Emerging Paradigm • The case of Israel • The challenge ahead • Potential solution Chernichovsky - draft - dov@mail.bgu.ac.il
Part A: The Emerging Paradigm (EP) Chernichovsky - draft - dov@mail.bgu.ac.il
From: Juan Luis Londoסo <jlondono@cable.net.co> To: "Dov Chernichovsky" <dov@bgumail.bgu.ac.il> References: <4.2.0.58.20010301093539.019e72a0@mail.bgu.ac.il> Subject: RE: Monograph Date: Sat, 3 Mar 2001 11:42:54 -0500 MIME-Version: 1.0 Content-Type: text/plain; charset="iso-8859-1" Content-Transfer-Encoding: 7bit X-Priority: 3 X-MSMail-Priority: Normal X-Mailer: Microsoft Outlook Express 5.00.2615.200 X-MimeOLE: Produced By Microsoft MimeOLE V5.00.2615.200 Dov: I lov e the idea. Lets do it!!! Juan Luis ----- Original Message ----- From: Dov Chernichovsky <dov@bgumail.bgu.ac.il> To: Juan Luis Londono <jlondono@cable.net.co>; W. van de Ven <vandeVen@ECON.BMG.eur.nl>; Elena Potapchik <elenap@4unet.ru> Sent: Thursday, March 01, 2001 2:43 AM Subject: Monograph > Dear Elena, Juan Luis, and Wynand: >…………….. >I propose editing a book "THE EMERGING PARADIGM IN HEALTH SYSTEMS; >COLOMBIA, ISRAEL, THE NETHERLANDS, AND RUSSIA. >The book would bring together our experiences under a unified analytic framework. >From what I > know the work exists by-and-large. We probably need to organize /edit it > around a set of common issues, highlighting how these are affected by the > backgrounds / circumstances in which the Paradigm has been implemented in > each of our nations. > What do you think? Further ideas /suggestions would be welcome. > Regards, >> Dov A Personal Note – Juan’s Response to the EP Chernichovsky - draft - dov@mail.bgu.ac.il
The Philosophical Foundation of the Paradigm Access to medical care is a right, almost regardless of its impact on health
Desired Social Qualities of the ‘Public’ System • Equity • Containment of medical expenditure growth • Production efficiency • Public (client) satisfaction Chernichovsky - draft - dov@mail.bgu.ac.il
The Policy and Structural Needs, to Meet the Qualities • Strengthen “state” cum “public” elements for • Equity • Cost-control • Strengthen “non-state” cum “competitive” for • Production efficiency • Client satisfaction Chernichovsky - draft - dov@mail.bgu.ac.il
Conceptual Challenges to Overcome, to meet the Needs • Break the dichotomy between private/competitive, on the one hand, and public-state/non-competitive, on the other • Or, break the vertical institutional integration of all system functions (mainly, finance and provision) • Disassociate between • “private” and “competitive”; private not a necessary condition for competition • “state” and “public”; state not a necessary condition for invoking and implementing public principles • Give rise to the concept of the “internal market” operating under the auspices of public finance principles Chernichovsky - draft - dov@mail.bgu.ac.il
Emerging System Organization and Management Principles -- Finance • Financing is based on public principles: Means-tested mandatory contributions, pooling of funds, and universal allocation • Contributions, potentially earmarked, not necessarily an integral part of the state’s budget • Emergence of the ‘true’ social insurance (national pool) model -- Western Continental Europe, Central and East Europe, Latin America Chernichovsky - draft - dov@mail.bgu.ac.il
Emerging System Organization and Management Principles -- Provision • Provision – when possible -is based on competitive principles , to achieve production efficiency and client satisfaction. These principles need not necessarily be implemented by private institutions operating in a free market • The push for provider “Trusts” -- UK and Eastern Europe Chernichovsky - draft - dov@mail.bgu.ac.il
Emerging System Organization and Management Principles -- OMCC • The natural emergence of fund-holding institutions that manage and organize care consumption (OMCCs) • Clearly defined entities in systems with recent strong legacies of private insurance insurance, e.g., Western Europe, and (fragmented) social insurance based on labor unions, e,g., Latin America • OMCC - the most unique feature of the Emerging Paradigm Chernichovsky - draft - dov@mail.bgu.ac.il
The Political-Economic Appeal of OMCC Institutions • To Government • Get out of care management, the least • Mechanism for financial risk sharing (vertical, with government) • Mechanism for risk pooling (horizontally, across groups) • To traditional insurers / sickness funds • Stay in the market • To labor unions • Keep a grip on the system or some elements • To everybody • Keep government out Chernichovsky - draft - dov@mail.bgu.ac.il
Emerging System Organization and Management Principles – Other Functions (Largely State) • Policy making and regulation • Health Promotion • Research and development • Human Resources development Chernichovsky - draft - dov@mail.bgu.ac.il
Part B: The Case of Israel Chernichovsky - draft - dov@mail.bgu.ac.il
Basic EP Features of 1995 Israeli Reform • Entitlement is universal and ‘standardized’; is implemented through • Means tested mandatory contributions • Pooling of all contributions, not through state budget • A universal risk adjusted allocation - capitation system • Compulsory enrollment in a sickness fund of choice • Sickness funds – intended to organize and manage all care -- compete in the first internal market on quality of care and service • Providers – intended to be free standing -- compete in second internal market on quality and fees Chernichovsky - draft - dov@mail.bgu.ac.il
Israeli System – Following 1995 Legislation Mexican 20?? Households State Employers Collection and Pooling Health Tax Parallel Tax General Contribution Finance Private Finance National Insurance Institute --- pool Universal Allocation - Capitation Competing Sickness Funds -- 1st internal market Issste Pemex OMCC IMSS MCH & Mental health Competing providers – 2nd internal market Provision State Hospitals Chernichovsky - draft - dov@mail.bgu.ac.il
OMCC designs in Israel Chernichovsky - draft - dov@mail.bgu.ac.il
Part C: The Challenges Ahead Chernichovsky - draft - dov@mail.bgu.ac.il
The Challenge Ahead • Empower at least high and middle income clients, without sacrificing “too much” equity and cost control • Keep (or mobilize) the rich or even middle class in (for) the public system Chernichovsky - draft - dov@mail.bgu.ac.il
The Issue Equity has come at the expense of transparency and consumer choice
The Tradeoffs and Backlash Conceptualized Backlash entitlement Chernichovsky - draft - dov@mail.bgu.ac.il
Context - Global • Fast income growth, combined with a widening income distribution • Fast technological advances, first available to higher income groups in private markets • “consumerism” in medical care • The definition of “medical care” is increasingly made by consumers Chernichovsky - draft - dov@mail.bgu.ac.il
Context – Israeli • Ministry of Finance under pressure to cut budgets • Not enough competition / diversity amongst sickness funds, to satisfy fast enough increasing demands for care Chernichovsky - draft - dov@mail.bgu.ac.il
The Results and Risks • Unholy alliance between high income groups, the profession, and ministries of finance, at least in Israel (1997/8 budget legislation) the fulled • Growth of supplemental insurance for ‘extra benfits’ • Growth of co-payments • Implicit sanctioning of private services in publicly supported provider institutions • Risks to governance, equity, and cost-containment Chernichovsky - draft - dov@mail.bgu.ac.il
Part D: Potential solution Chernichovsky - draft - dov@mail.bgu.ac.il
Use the OMCCs for a Solution • Resolve the schizophrenic “agent” problem: • Government represents contributors • OMCCs represent clients – giving these institutions a distinct role • Providers represent providers • Allow free group choice of entitlement within a pre-set public budget, beyond a publicly mandated core minimum • Allow alternative modes of providing any given entitlement • Establish new links with the private sector Chernichovsky - draft - dov@mail.bgu.ac.il
Proposed Organization and Finance of Entitlement Private entitlement and finance OMCC or Group-specific public entitlement, financed by a pre-set portion of public-based finance Public-based OMCC Core public entitlement – common to all groups Chernichovsky - draft - dov@mail.bgu.ac.il
The Health System A Corporate Federation of Consumer-based Entities, Paid by the Public, With Some Basic Constitutional Rights About the Nature of Care They Consume Chernichovsky - draft - dov@mail.bgu.ac.il
References Chernichovsky, D. and Chinitz, D. “The Political Economy of Health System Reform in Israel”. Health Economics 1995. Vol. 4: 127-141. Chernichovsky, D. “What Can Developing Economies Learn from Developed Economies?” Health Policy 1995. Vol. 32: 79-91 Chernichovsky, D. “Health System Reforms in Industrialized Economies; An Emerging Paradigm. The Milbank Quarterly 1995. Vol. 73, no. 3: 339-372 Chernichovsky, D. “Pluralism, Choice, and the Sate in the Emerging Paradigm in Health Systems.” The Milbank Quarterly. 2002. Vol. 80, no. 1:5-40. Shmueli, A., Chernichovsky and I. Zmora. “Risk adjustment and risk sharing: the Israeli experience”. Health Policy. 2003. Vol. 65, no. 1:37-48 Chernichovsky, D. “The Americanization of the Israeli Health Care System” (Processed) Chernichovsky - draft - dov@mail.bgu.ac.il