Download
1 / 57
580 likes | 747 Views
Prostate Problems. By Dr Mahya Mirfattahi GPST1 HDR Wednesday 17 th February 2010. Lower urinary tract symptoms. Obstructive Poor stream, hesistancy, terminal dribbling, pis-en-deux (incomplete bladder empyting), overflow incontinence Irritative Frequency, nocturia, urgency, dysuria.

E N D
ProstateProblems By Dr Mahya Mirfattahi GPST1 HDR Wednesday 17th February 2010
Lower urinary tract symptoms • Obstructive • Poor stream, hesistancy, terminal dribbling, pis-en-deux (incomplete bladder empyting), overflow incontinence • Irritative • Frequency, nocturia, urgency, dysuria
Case 1 - 60 yr old male • Describes difficulty starting and stopping when urinating with a poor stream • Compelled to void again soon after going • Getting up during night average 3x • PMH – Hypertension • What else would you like to know?
Aims of history • Assess symptoms & severity • Assess impact on quality of life • Identify other causes of LUTS • Identify complications • Identify co-morbidities that may complicate treatment
Case 1: Exploring things further • 6/12 Hx gradual worsening symptoms • Worries when out & about – always looking for toilet • No dysuria or haematuria • No Hx of incontinence • Thinks is part of ageing! • DH – Amlodipine 5mg
IPSS (International Prostate Symptom Score) • Objective measurement to grade symptoms • Useful to quantify severity, help to choose appropriate treatment & monitoring response • Mild = 0-7, Moderate = 8-19, Severe 20-35 • Only 20% of GPs use this • Should we be using it more often?
Differential Diagnosis for LUTS • Causes of outflow obstruction • BPH, urethral stricture, severe phimosis, idiopathic bladder outlet obstruction, bladder neck or sphincter dyssynergia • Inflammatory conditions • UTI, bladder stone, prostatitis, interstitial cystitis • Neoplastic • Bladder or prostate cancer
DD continued • Bladder storage disorders • Overactive bladder syndrome, underactive detrusor • Neurological conditions • MS, Parkinson’s, CVA • Conditions causing polyuria • Diabetes, congestive cardiac failure
Case 1 - Examination • What would you like to do? • DRE – anal tone, size of prostate & abnormalities (hard, nodular, irregular, or fixed = carcinoma vs. smooth & regular) • Focused neurological examination • Abdominal examination • Distended palpable bladder or other causes e.g. abdominal/pelvic mass
Case 1 – Investigations • PSA – more on this later! • Urinalysis • Exclude UTI, haematuria, glucose • Renal function tests • All patients presenting with LUTS • If renal impairment needs renal USS to check for hydronephrosis • Flow rate studies • Can be helpful to confirm diagnosis, objectively measure severity, monitor response to treatment • QMax & post void residual volume
Case 1 - Management • You diagnose mild BPH with no complications, what treatment option(s) will you discuss? • Watchful waiting • As not severely troubled by symptoms • Advise reducing fluid intake particularly caffeine & alcoholic drinks • Review medications e.g. diuretics • Preventing constipation • Advise to return if symptoms deteriorate
Treatment of BPH • Aims of treatment are • Relieve symptoms • Improve quality of life • Attempt to prevent progression of disease & development of complications
Case 1 – He returns 3/12 later • Symptoms worsened • Embarrassing episodes of urge incontinence • Worries about leaving the house • Wants to try medical therapy now • He has heard of using saw palmetto & wants to know if this is ok to try • What can we offer him?
Medical therapy – the options • Alpha antagonists = 1st line • Work by relaxing smooth muscle in prostate & reduces urinary outflow resistance • Benefits • Act rapidly usually 48hrs, symptomatic relief immediately noticeable • 70% respond to treatment, expected in 3/52 • Evidence • Many RCT & systematic review – similar efficacy between drugs & formulations • Choice dependant on tolerability & those with pre-existing cardiovascular co-morbidity or co-medication
Alpha antagonist continued • Side effects • Cardiovascular – postural hypotension, dizziness, headaches • GU – failure of ejactulation • CNS – somnolence, dizziness • Compliance better with newer once daily sustained release e.g. Flomax MR, Xatral XL • No effect on prostate volume • Recommendations • Suitable for moderate-severe LUTS, low risk of disease progression • Tamsulosin has best cardiovascular side effect profile = 1st line • Alfuzosin
5-alpha reductase inhibitors • Reduces production of dihydrotestosterone & arrests prostatic hyperplasia • Two licensed for use in UK • Finasteride (Proscar) • Dutasteride (Avodart) • Similar clinical efficacy & safety profile • Warn patients that shrinkage takes time – 6/12 & no noticeable symptom improvement for this period • Side effects • ED, loss of libido, ejaculatory disorders, gynaecomastia, breast tenderness • Recent drug alert issue – link to male breast cancer
5-alpha reductase inhibitors continued • Recommendations • Suitable for moderate-severe LUTS & obviously enlarged prostate & those more likely to have progressive disease • NB – reduces PSA levels by half – need to adjust when interpreting results for suspected prostate cancer • Risk factors for disease progression • Age >70yrs, IPSS >7, Prostate volume >30mls, PSA level >1.4ng/ml, QMax <12ml/s, Post void RV >100mls
Combination therapy • For those patients with increased risk of disease progression & symptomatic • Increased side effects
Alternative therapies • Remember the saw palmetto • Is a plant extract • Others: Pumpkin seeds, stinging nettle root, cactus flower extracts, South African star grass, African plum tree • Currently NOT recommended (be aware of Oxford Handbook of GP) • Advise patient • Although some evidence in studies shows benefits LUTS, it has not undergone same scrutiny for efficacy, purity or safety
Case 2 – 70 yr old male • Presents with painful inability to pass urine • Has tried several times to go without success since last night • No Hx of voiding difficulties • No back pain/sciatica • Has been constipated last few days • PMH - Osteoarthritis
What is your diagnosis & management? • He has a palpable bladder • DRE – large prostate, normal perineal sensation & anal tone • Acute urinary retention • This is urological emergency • Admit for catheterisation
When to refer in BPH? • Based on NICE guidelines • Urgent if • Acute or chronic urinary retention • Renal failure • Any suspicion of neurological dysfunction • UCR • Haematuria – see next presentation • Suspected malignant prostate • Soon • Recurrent UTI • Routine • Unclear diagnosis • No improvement on initial medical therapy
Case 3 – 50 yr old male • Presents with dysuria, frequency & urgency symptoms • Feverish • Low back pain • Suprapubic pain • Perineal pain • Painful to open bowels • PMH: Type 2 Diabetes, Angina
What’s your DD? • UTI • Acute prostatitis • Urethritis • Cystitis • Pyelonephritis • Acute epididymo-orchitis • Local invasion from prostate, bladder or rectal cancer
Clinical assessment • Temp 37.8 • Abdomen – soft, tender suprapubic, no loin tenderness • Urine dipstick +ve leucocytes & nitrites • DRE – Tender prostate • You diagnose acute prostatitis & discuss with urology for urgent referral
Treatment of Acute Prostatitis • Start antibiotics immediately (whilst waiting MSU results) • Ciprofloxacin 500mg BD • Ofloxacin 200mg BD • Treat for 28 days (prevent chronic prostatitis) • If neither above tolerated, trimethoprim 200mg BD for 28 days • Quinolones or trimethoprim effective in most of likely pathogens & high concentrations in prostate • If unable to take oral Abx or severely ill - admit
Treatment continued • Treat pain • Paracetamol +/- ibuprofen = 1st line • If severe offer codeine • If defecation painful offer stool softener – recommended: lactulose or docusate • Advise to seek medical advice if deteriorates • Reassess in 24-48hrs • Review culture results & ensure appropriate Abx • Refer to urology if not responding adequately to treatment, consider prostate abscess
Acute Prostatitis • Potentially serious bacterial infection of prostate • Urinary pathogens = culprits commonly • Gram –ve organisms e.g. E.coli, proteus sp, klebsiella, pseudomonas • Enterococci • Accompanied by UTI, occasionally epididymitis or urethritis • Not sexually transmitted • Can follow urethral instrumentation, trauma, bladder outflow obstruction, dissemination of infection from elsewhere
Referral • Admit • If acute urinary retention, will need suprapubic catheterisation • Deteriorating symptoms despite appropriate Abx, need to exclude prostatic abscess (transrectal USS or CT) • Urgent • If pre-existing urological condition e.g. BPH, or indwelling catheter • Immunocompromised or diabetic • Consider referral when recovered –investigation to exclude structural abnormality
Case 3 continued • 6/12 later he returns with continuing pain in perineum • Also complains of painful ejaculation affecting relationship • Still getting some LUTS – mainly frequency, urgency and poor stream • General aches in pelvis – fluctuates, deep, and sometimes in lower back • Tired, getting him down
What will you do next? • Physical examination • Exclude other diagnosis • DRE: diffusely tender prostate • Urine culture • Consider PSA – more on this later • Prostatic massage not recommended in primary care
Diagnosis = Chronic Prostatitis • Characterised by at least 3/12 of pain in perineum or pelvic floor • Often with LUTS • Dysuria, frequency, hesitancy & urgency • And sexual dysfunction • ED, painful ejaculation, post-coital pelvic discomfort • Can be divided into 2 types • Chronic bacterial = 10% • Chronic pelvic pain syndrome = 90% • Management in primary care not dependent on classification
Management of Chronic Prostatitis • Assess severity of pain, urinary symptoms & impact on quality of life • Reassurance not cancer & not STI • Trend is for symptoms to improve over months-years • If defecation painful: offer stool softener • Consider trial of paracetamol +/- ibuprofen for 1/12 • If Hx of UTI (or episode of acute prostatitis) in last 12 mo consider single course of antibiotic • Quinolone for 28 days, or trimethoprim where not tolerated
Referral • Refer cases to urology • Can start Abx whilst awaiting review • Urologist may consider trial of alpha blocker for 3/12 • Consider chronic pain specialist referral
Case 4 – 68 yr old, male • Presents with wife requesting PSA test • No symptoms • Concerns as advancing age • Has friends in USA of similar age that are screened for prostate cancer annually • Asking if similar NHS screening programme • PMH: Hypertension, low back pain
How will you approach this request? • Back to basics – history & examination • Ask about LUTS, sexual dysfunction, ICE(!) • Red flags: Weight loss, bone pain, haematuria • DRE: Hard, irregular prostate, loss of sulcus, palpable seminal vesicle
ICE is helpful • He is concerned about prostate cancer • Because there is a family Hx • Assessing risk: • If one 1st degree relative <70yr: RR 2 • Two 1st degree relatives (one of them) <65: RR 4 • Three or more relatives: RR 7-10 • Risk factors • Increasing age (85% diagnosed >65yrs) • Ethnicity: highest rates in black ethnic group (lowest Chinese) • Diet: Evidence that high in dairy products & red meat linked to increased risk
PSA testing counselling • There is no prostate screening programme in the UK • Men can request a PSA test • www.cancerscreening.nhs.uk = good website with pt info leaflet
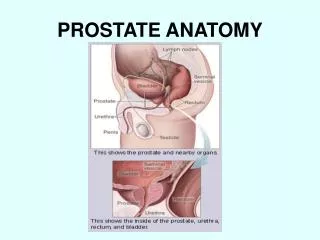
Things to tell patients • What is prostate cancer? • Gland lies beneath bladder • Each yr 22,000 men are diagnosed with prostate cancer • Rare in men <50yrs • Average age of diagnosis is 75yrs • Slow growing cancers are more common than fast growing ones –no way of telling between two • May not cause symptoms or shorten life
Things to tell patients (2) • What is the PSA test? • Blood test • Many causes of raised levels • 2/3 of men with raised PSA do NOT have cancer • May lead to unnecessary anxiety and further investigations when no cancer is present • Can provide reassurance if normal • May miss diagnosis too (false reassurance) • Does not distinguish between aggressive and non-aggressive tumours • May detect early stage of cancer when treatments could be beneficial
Things to tell patients (3) • If raised, examine to check prostate or repeat test in few months • If referral to specialist • Prostate biopsy (TRUS) • Complications – uncomfortable, bleeding & infection • 2 out of 3 men who have prostate biopsy will not have prostate cancer • However, biopsies can miss some cancers
Things to tell patients (4) • Treatment options • Depends on classification (localised to prostate, locally advanced, metastatic) • No strong evidence to suggest treatment of localised cancer reduces mortality • Main treatments have significant side effects & no certainty that treatments will be successful
PSA test practicalities • Before PSA men should not have • Active UTI (wait 1/12) • DRE (in previous week) • Recent ejaculation (previous 48hrs) • Vigorous exercise (previous 48hrs) • Prostate biopsy (previous 6/12)
Problems with PSA screening • A good screening test should fulfil Wilson-Jungner Criteria (1968, WHO) • The only criterion met = prostate cancer is important health problem • No good understanding of natural history of condition, no acceptable level of sensitivity or specificity of test, no clear demonstrable benefit of early treatment
Problems with PSA screening • No means to detect which ‘early’ cancers become more widespread • More men would be found with prostate cancer than would die or have symptoms from it • Not clear if early treatment enhances life expectancy • No strong evidence that PSA testing reduces mortality from prostate cancer
Case 4 continued • PSA = 4.5 ng/ml • DRE – hard craggy prostate • What will you do? • UCR referral • DRE: hard irregular prostate typical of prostate cancer. Include PSA result with referral • DRE: normal prostate, but rising/raised age-specific PSA with or without LUTS • Symptoms & high PSA levels • Asymptomatic men with borderline age-specific PSA rpt test after 1-3 mo. If still rising refer.
Threshold PSA levels • Age-related referral values for total PSA levels recommended by the Prostate Cancer Risk Management Programme • AgePSA referral value (ng/ml) • 50–59 ≥ 3.0 • 60–69 ≥ 4.0 • 70 and over > 5.0
Case 4 continued • His Gleason score =7 • What does this mean? • Moderate chance of cancer spreading • Gleason score characterises prostate cancers on basis of histological findings • Used with T part of TNM staging to stratify risk of risk of progression
Treatment options • Watchful waiting • Low risk patients • Monitoring with annual PSA/rectal examination • Increase in PSA or size of nodule triggers active treatment