Download
1 / 25
270 likes | 629 Views
PROSTATE INFECTION. Acute Bacterial Prostatitis Chronic Bacterial Prostatitis Granulomatous Prostatitis Prostate Abscesss. PROSTATE INFECTION. Acute Bacterial Prostatitis Chronic Bacterial Prostatitis Granulomatous Prostatitis Prostate Abscesss. Acute Bacterial Prostatitis.

E N D
PROSTATE INFECTION Acute Bacterial Prostatitis Chronic Bacterial Prostatitis GranulomatousProstatitis Prostate Abscesss
PROSTATE INFECTION Acute Bacterial Prostatitis Chronic Bacterial Prostatitis GranulomatousProstatitis Prostate Abscesss
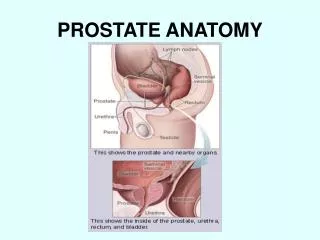
Acute Bacterial Prostatitis • inflammation of the prostate associated with a UTI. • It is thought that infection results from ascending urethral infection or reflux of infected urine from the bladder into the prostatic ducts
Acute Bacterial Prostatitis • uncommon in prepubertal boys but frequent affects adult men • most common urologic diagnosis in men younger than 50 years • Clinical presentation: • present with an abrupt onset of constitutional • Fever, chills, malaise, arthralgia, myalgia, lower back/rectal/perineal pain • urinary symptoms (frequency, urgency, dysuria) • Urinary retention due to swelling of the prostatate • DRE: tender, enlarged glands that are irregular and warm
Acute Bacterial Prostatitis • Laboratory findings: • Urinalysis : WBCs and occasionally hematuria • Serum blood analysis: leukocytosis • Prostate-specific antigen levels: elevated • Culture of urine and prostate expressate: usually single oragnismbut occasionally, polymicrobialinfection may occur. • Pathogens: • E. Coli: most common • Gram negative bacteria: Proteus, Klebsiella, Enterobacter, Pseudomonas, and Serratia spp., enterococci – less frequent • Anaerobic and other gram-positivebacteria-rare
Acute Bacterial Prostatitis • Management: • Empiric therapy against Gram negative bacteria Enterococci, immediately while awaiting for culture results • Trimethoprim and fluoroquinolones • Ampicillinand an aminoglycoside • effective therapy against both gram-negative bacteria and enterococci
PROSTATE INFECTION Acute Bacterial Prostatitis Chronic Bacterial Prostatitis GranulomatousProstatitis Prostate Abscesss
PROSTATE INFECTION Acute Bacterial Prostatitis Chronic Bacterial Prostatitis GranulomatousProstatitis Prostate Abscesss
Chronic Bacterial Prostatitis • In contrast to the acute form, chronic bacterial prostatitis has: • a more insidious onset, characterized by relapsing, recurrent UTI caused by the persistence of pathogen in the prostatic fluid despite antibiotic therapy.
Chronic Bacterial Prostatitis • Clinical Presentation: • dysuria, urgency, frequency, nocturia, and low back/perinealpain • Afebrile • not uncommonly have a history of recurrent or relapsing UTI, urethritis, or epididymitis caused by the same organism • asymptomatic, but the diagnosis is made after investigation for bacteriuria • DRE: normal; occasionally, tenderness, firmness, or prostatic calculi may be found on examination
Chronic Bacterial Prostatitis • Laboratory findings: • Urinalysis: variable degree of WBC &bacteria • Serum blood analysis: no leukocytosis • Prostate-specific antigen levels: elevated • Diagnosis is made after • causative oragnisms: • similar to those of acute bacterial prostatitis • other gram-positive bacteria: • Mycoplasma, Ureaplasma, and Chlamydia spp. are not causative pathogens in chronic bacterial prostatitis.
Chronic Bacterial Prostatitis • Diaganosis is made after the identification of bacteria from prostate expressate or urine • specimen after a prostatic massage, using the 4-cup test
Chronic Bacterial Prostatitis • Management: • Similar to acute bacterial prostatitis • duration of antibiotic therapy: 3–4 months. • Using fluoroquinolones, some patients may respond after 4–6 weeks of treatment. • addition of an alpha blocker to antibiotic therapy has been shown to reduce symptom recurrences
Chronic Bacterial Prostatitis • Recurrent episodes of infection occur despite antibiotic therapy: • TMP-SMX 1 single-strength tablet daily • Nitrofurantoin100 mg daily, or • ciprofloxacin 250 mg daily • Transurethral resection of the prostate has been used to treat patients with refractory disease; however, the success rate has been variable and this approach is not generally recommended
PROSTATE INFECTION Acute Bacterial Prostatitis Chronic Bacterial Prostatitis GranulomatousProstatitis Prostate Abscesss
PROSTATE INFECTION Acute Bacterial Prostatitis Chronic Bacterial Prostatitis GranulomatousProstatitis Prostate Abscesss
GranulomatousProstatitis • uncommon form of prostatitis • can result from bacterial, viral, or fungal infection, the use of bacillus Calmette-Guerin therapy • malacoplakia, or systemic granulomatousdiseases affecting the prostate
GranulomatousProstatitis • Clinical Presentation: • acutely, with fever, chills, and obstructive/irritativevoiding symptoms • Some with urinary retention • eosinophilicgranulomatousprostatitis –severely ill with high fevers • DRE: hard, indurated, and fixed prostate, which is difficult to distinguish from prostate carcinoma.
GranulomtaousProstatitis • Laboratory findings: • Urinalysis and culture: • do not show any evidence of bacterial infection • Serum blood analysis – leukocytosis, marked eosinophilia in patients with eosinophilic type • The diagnosis is made after biopsy of the prostate.
GranulomatousProstatitis • Management: • Some patients respond to antibiotic therapy, corticosteroidsand temporary bladder drainage. • Transurethral resection of the prostate may be required in patients who do not respond to treatment and have significant outlet obstruction.
PROSTATE INFECTION Acute Bacterial Prostatitis Chronic Bacterial Prostatitis GranulomatousProstatitis Prostate Abscesss
PROSTATE INFECTION Acute Bacterial Prostatitis Chronic Bacterial Prostatitis GranulomatousProstatitis Prostate Abscesss
Prostate Abscess • complications of acute bacterial prostatitis that were inadequately or inappropriately treated. • Seen in patient : • diabetes • chronic dialysis patients • Immunocompromised • chronic indwelling catheters
Prostate Abscess • Clinical Presentation: • similar symptoms to those with acute bacterial prostatitis. • these patients were treated for acute bacterial prostatitis previously and had a good initial response to treatment with antibiotics. • However, their symptoms recurred during treatment, suggesting development of prostatic abscesses. • DRE: prostate is usually tender and swollen
Prostate Abscess • Management: • Antibiotic therapy in conjunction with drainage of the abscess is required • Transrectalultrasonography or CT scan can be used to direct transrectal drainage of the abscess • Transurethral resection and drainage may be required if transrectal drainage is inadequate. • When properly diagnosed and treated, most cases of prostatic abscess resolve without significant sequelae